cybrsage
New member
I have a bottle of YK11 in the mail - yes, I am one of the bleeding edge type of people. ") I figure that since GW50 is helping me so fantastically (I have a log on it for those who missed it - you can find it here: ), what can YK11 do for me? I bought a bottle of YK11 from SarmsSearch and will be running it at 5mg/day once I receive it. I will even post a pretty picture of it when it arrives.
I figure that since GW50 is helping me so fantastically (I have a log on it for those who missed it - you can find it here: ), what can YK11 do for me? I bought a bottle of YK11 from SarmsSearch and will be running it at 5mg/day once I receive it. I will even post a pretty picture of it when it arrives.
YK11 is very bleeding edge, in other words, it is very new and no one really knows dosing yet. Bro-science says to start at 5mg and up to 10mg after a week if you are seeing no bad side effects and/or you are not seeing the good effects. Thusly, I will be following the bro-science - but only because there is no real science yet to guide us.
I posted this already, but it will be served well to repost it here. Here is the real science we DO know about YK11.
OK, having done a bunch of reading, this is what I understand about YK11:
YK11 stimulates the creation of follistatin. When YK11 is in the presence of follistatin, it causes a large sudden production of myogenic differentiation factor (MyoD), myogenic factor 5 (Myf5) and myogenin. The three myogenic items are what causes the body to create new muscle cells. Testosterone and DHT compounds also do this, but without the creation or need for follistatin. Well, not quite correct, testosterone does induce the creation of follistatin, just not nearly at the same level as YK11. Normally, the body produces myostatin as a counter to mygenin (it competes for the same receptors and then encourages the body to destroy the newly created muscle cells), to help keep the body from just making more and more muscle (which is normally what we want). Follistatin aids in the reducing the effect of myostatin in a few ways, but that is outside the scope of what I am talking about. It is this follistatin that makes YK11 so powerful compared to testosterone or DHT compounds (and why testosterone is still a better choice for muscle creation than other AAS - it is a perfect item to use in synergy with other items).
The human body, being an insanely amazing thing, is not powerless against follistatin. As follistatin levels rise, it creates an anti-follistatin antibody. This anti-body helps restore the body back to its normal state so there is not run-away muscle creation (again, that would be a bad thing).
YK11 is only partially androgenic and it has the same effects on FKBP51 as DHT compounds do, in other words, it increases it quite a bit. This is only a problem if you currently have cancer, as FKBP51 is instrumental in cell survival and it will also greatly aid cancer cells in their survival. If you have cancer, do not take YK11...and also do not take any compound that turns into DHT in the body. Yeah, that is just about every good AAS out there. Remember, cancer is no joke, so if you have it, getting rid of it should be your number one priority...not gaining muscle. Don't be a loser about it and die just to look good at your funeral. For the vast majority of people without cancer, there is no problem with having an increased FKBP51 level. Increased FKBP51 levels does NOT cause cancer.
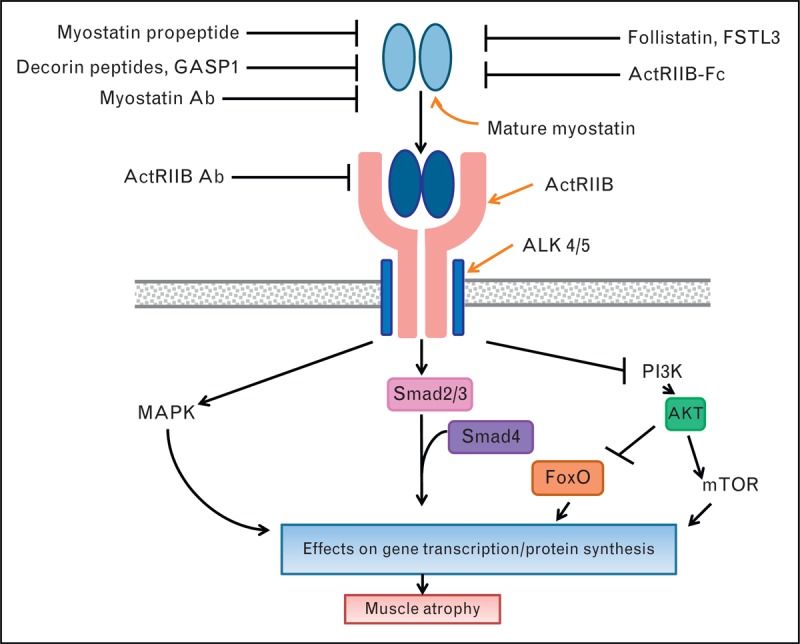
I have found no side effects at all for YK11 (other than the increase in FKBP51, which you also find in most AAS), but it is still a very new SARM so only time will tell. There is also no suggested dosing by the medical community, again due to it being so new. As far as I can tell, it has yet to be used on a live creature by the medical community - it has only been used on cell cultures. At least they were human cell cultures. Welcome to the bleeding edge here folks! I have included a nice picture showing that follistatin and myostatin compete for the same receptors. Myostatin encourages muscle atrophy, follistatin encourages muscle creation (more or less correct for both).
View attachment 563306
YK11 also does not appear to cause the creation of Estrogen - it appears to do the same thing as Tamoxifen (though through a completely different method) but to a far lesser degree. YK11 cannot be used as a SERM replacement so please do not try.
What we need to keep an eye out for is nosebleeds. ACE31 was a myostatin inhibitor with great promise, made it into phase 2 human trials where they tested it on both people with muscular dystrophy and healthy people. It caused bad nosebleeds that stopped when the drug was no longer taken. It has been shelved until someone can figure out how to stop the bleeding. Since YK11 also appears to inhibit myostatin (though through completely different mechanisms), there is always the chance it will cause nosebleeds as well. They have no idea why ACE31 causes nosebleeds, but it did it with enough power and frequency to kill what looked like a huge money maker for the big pharma developing it. I doubt YK11 will cause nosebleeds, due to the way it works, but it is better to keep an eye out for it and it never happen than it to happen and you think it is caused by the change in seasons.
For me, YK11 looks like something I would like to try out. I think it, combined with a good AAS regimen, could help push me to greater heights.
Sources:
https://www.jstage.jst.go.jp/article/bpb/36/9/36_b13-00231/_html
Biol. Pharm. Bull. 34(3) 318***8212;323 (2011) Vol. 34, No. 3 (17a,20E)-17,20-[(1-Methoxyethylidene)bis(oxy)]-3-oxo-19-norpregna-4,20-diene-21-carboxylic Acid Methyl Ester (YK11) Is a Partial Agonist of the Androgen Receptor
As soon as I have it in hand, the logging will begin. Or at least within a few days of it.
I figure that since GW50 is helping me so fantastically (I have a log on it for those who missed it - you can find it here: ), what can YK11 do for me? I bought a bottle of YK11 from SarmsSearch and will be running it at 5mg/day once I receive it. I will even post a pretty picture of it when it arrives.YK11 is very bleeding edge, in other words, it is very new and no one really knows dosing yet. Bro-science says to start at 5mg and up to 10mg after a week if you are seeing no bad side effects and/or you are not seeing the good effects. Thusly, I will be following the bro-science - but only because there is no real science yet to guide us.
I posted this already, but it will be served well to repost it here. Here is the real science we DO know about YK11.
OK, having done a bunch of reading, this is what I understand about YK11:
YK11 stimulates the creation of follistatin. When YK11 is in the presence of follistatin, it causes a large sudden production of myogenic differentiation factor (MyoD), myogenic factor 5 (Myf5) and myogenin. The three myogenic items are what causes the body to create new muscle cells. Testosterone and DHT compounds also do this, but without the creation or need for follistatin. Well, not quite correct, testosterone does induce the creation of follistatin, just not nearly at the same level as YK11. Normally, the body produces myostatin as a counter to mygenin (it competes for the same receptors and then encourages the body to destroy the newly created muscle cells), to help keep the body from just making more and more muscle (which is normally what we want). Follistatin aids in the reducing the effect of myostatin in a few ways, but that is outside the scope of what I am talking about. It is this follistatin that makes YK11 so powerful compared to testosterone or DHT compounds (and why testosterone is still a better choice for muscle creation than other AAS - it is a perfect item to use in synergy with other items).
The human body, being an insanely amazing thing, is not powerless against follistatin. As follistatin levels rise, it creates an anti-follistatin antibody. This anti-body helps restore the body back to its normal state so there is not run-away muscle creation (again, that would be a bad thing).
YK11 is only partially androgenic and it has the same effects on FKBP51 as DHT compounds do, in other words, it increases it quite a bit. This is only a problem if you currently have cancer, as FKBP51 is instrumental in cell survival and it will also greatly aid cancer cells in their survival. If you have cancer, do not take YK11...and also do not take any compound that turns into DHT in the body. Yeah, that is just about every good AAS out there. Remember, cancer is no joke, so if you have it, getting rid of it should be your number one priority...not gaining muscle. Don't be a loser about it and die just to look good at your funeral. For the vast majority of people without cancer, there is no problem with having an increased FKBP51 level. Increased FKBP51 levels does NOT cause cancer.
I have found no side effects at all for YK11 (other than the increase in FKBP51, which you also find in most AAS), but it is still a very new SARM so only time will tell. There is also no suggested dosing by the medical community, again due to it being so new. As far as I can tell, it has yet to be used on a live creature by the medical community - it has only been used on cell cultures. At least they were human cell cultures. Welcome to the bleeding edge here folks! I have included a nice picture showing that follistatin and myostatin compete for the same receptors. Myostatin encourages muscle atrophy, follistatin encourages muscle creation (more or less correct for both).
View attachment 563306
YK11 also does not appear to cause the creation of Estrogen - it appears to do the same thing as Tamoxifen (though through a completely different method) but to a far lesser degree. YK11 cannot be used as a SERM replacement so please do not try.
What we need to keep an eye out for is nosebleeds. ACE31 was a myostatin inhibitor with great promise, made it into phase 2 human trials where they tested it on both people with muscular dystrophy and healthy people. It caused bad nosebleeds that stopped when the drug was no longer taken. It has been shelved until someone can figure out how to stop the bleeding. Since YK11 also appears to inhibit myostatin (though through completely different mechanisms), there is always the chance it will cause nosebleeds as well. They have no idea why ACE31 causes nosebleeds, but it did it with enough power and frequency to kill what looked like a huge money maker for the big pharma developing it. I doubt YK11 will cause nosebleeds, due to the way it works, but it is better to keep an eye out for it and it never happen than it to happen and you think it is caused by the change in seasons.
For me, YK11 looks like something I would like to try out. I think it, combined with a good AAS regimen, could help push me to greater heights.
Sources:
https://www.jstage.jst.go.jp/article/bpb/36/9/36_b13-00231/_html
Biol. Pharm. Bull. 34(3) 318***8212;323 (2011) Vol. 34, No. 3 (17a,20E)-17,20-[(1-Methoxyethylidene)bis(oxy)]-3-oxo-19-norpregna-4,20-diene-21-carboxylic Acid Methyl Ester (YK11) Is a Partial Agonist of the Androgen Receptor
As soon as I have it in hand, the logging will begin. Or at least within a few days of it.
