You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Basic Overview On Peptides
- Thread starter vibrant
- Start date
vibrant
CHEMICALLY ENGINEERED
Growth Hormone Releasing Peptide (GHRP-6) is a peptide in the growth factor family. It has strong effect on the release of Human Growth Hormone (HGH) in a specific and dose-related manner. GHRP can be effectively used in the treatment of growth hormone (GH) deficiency. Growth hormone releasing hexapeptide works by signaling the pituitary gland to begin growth hormone secretion.
Increased GH and IGF-1 levels are desirable for those looking to improve physique. Human growth hormone has been known to enhance immune response and stimulate the immune system, particularly older subjects. Dosed at night for anti-aging purposes and multiple times throughout the day for anabolism. GHRP is often used in conjunction with GHRH cjc-1295 to amplify growth hormone pulse. Avoid fats and carbohydrate a half hour on each side of dosing GHRP-6.
Bodybuilders and athletes utilize GHRP in an effort to build more muscle and burn fat. Some GHRP-6 users include it in their post cycle therapy (PCT). Cycling GHRP-6 in the off weeks from IGF/GH cycles is also becoming prevalent. Researchers wish to kick-start their body into producing their own natural GH & IGF, while gaining as if they remained on the GH/IGF peptides.
GHRP-6's main use is to promote food intake by stimulating hunger and aid in energy metabolism. The major side effect being a significant increase in appetite due to a stimulating the release of Ghrelin (about 20 minutes post injection), a hormone released naturally in the lining of the stomach and increases hunger and gastric emptying. This is why GHRP-6 can be used in the treatment of cachexia (wasting), eating disorders and obesity.
Benefits of increased HGH levels through GHRP-6 stimulation include: an increase in strength, muscle mass and body fat loss, rejuvenation and strengthening of joints, connective tissue and bone mass. Enhanced HGH secretion also leads to the liver secreting more IGF-1, which is thought to be the primary anabolic mechanism of action for Growth Hormone.
GHRP-6 5MG Peptide:
Mixing: Bacteriostatic water is used for reconstitution. When diluted, peptide lasts a very long time when left alone in the refrigerator (months)
Example- 2.5ml(cc) bacteriostatic water per 5mg GHRP vial equates to a 100mcg dose approximately each 2-3 marks on a U100 insulin syringe.
Example- 5ml(cc) bacteriostatic water per 5mg GHRP vial equates to a 100mcg dose approximately every 5 marks on a U100 insulin syringe.
Dosing: The saturation dose of GHRP-6 has been determined to be around 100mcg. More is not better in regards to this secretalogue
5mg GHRP = 5,000mcg
5,000mcg/100mcg = 50 100mcg GHRP doses per 5mg
GHRP-6 may be the most cost effective growth peptide available.
Increased GH and IGF-1 levels are desirable for those looking to improve physique. Human growth hormone has been known to enhance immune response and stimulate the immune system, particularly older subjects. Dosed at night for anti-aging purposes and multiple times throughout the day for anabolism. GHRP is often used in conjunction with GHRH cjc-1295 to amplify growth hormone pulse. Avoid fats and carbohydrate a half hour on each side of dosing GHRP-6.
Bodybuilders and athletes utilize GHRP in an effort to build more muscle and burn fat. Some GHRP-6 users include it in their post cycle therapy (PCT). Cycling GHRP-6 in the off weeks from IGF/GH cycles is also becoming prevalent. Researchers wish to kick-start their body into producing their own natural GH & IGF, while gaining as if they remained on the GH/IGF peptides.
GHRP-6's main use is to promote food intake by stimulating hunger and aid in energy metabolism. The major side effect being a significant increase in appetite due to a stimulating the release of Ghrelin (about 20 minutes post injection), a hormone released naturally in the lining of the stomach and increases hunger and gastric emptying. This is why GHRP-6 can be used in the treatment of cachexia (wasting), eating disorders and obesity.
Benefits of increased HGH levels through GHRP-6 stimulation include: an increase in strength, muscle mass and body fat loss, rejuvenation and strengthening of joints, connective tissue and bone mass. Enhanced HGH secretion also leads to the liver secreting more IGF-1, which is thought to be the primary anabolic mechanism of action for Growth Hormone.
GHRP-6 5MG Peptide:
Mixing: Bacteriostatic water is used for reconstitution. When diluted, peptide lasts a very long time when left alone in the refrigerator (months)
Example- 2.5ml(cc) bacteriostatic water per 5mg GHRP vial equates to a 100mcg dose approximately each 2-3 marks on a U100 insulin syringe.
Example- 5ml(cc) bacteriostatic water per 5mg GHRP vial equates to a 100mcg dose approximately every 5 marks on a U100 insulin syringe.
Dosing: The saturation dose of GHRP-6 has been determined to be around 100mcg. More is not better in regards to this secretalogue
5mg GHRP = 5,000mcg
5,000mcg/100mcg = 50 100mcg GHRP doses per 5mg
GHRP-6 may be the most cost effective growth peptide available.
vibrant
CHEMICALLY ENGINEERED
Insulin-like Growth Factor LR3 (IGF-1)
IGF-1 (Long R3 IGF-1) Dose:
Light: 25 mcg
Common: 50 mcg
Large: 100 mcg
IGF-1 is administered for one month, give or take a week.
Insulin-like Growth Factor (Long-R3 IGF-1), an 83 amino acid analog of IGF-1 is a highly anabolic hormone released primarily in the liver with the stimulus of growth hormone (HGH).
IGF-1 is the most potent growth factor found in the body and causes muscle cell hyperplasisa.
Freeze dried (lyophilized) IGF-1 (in powder state) should be stored in the freezer (-18 degrees celsius).
Dilute the IGF-1 peptide with 2mls of Acetic Acid (.6%). Assuming (*DO NOT ASSUME*) Acetic Acid (AA) will yield the correct pH balance of your research peptide.
Note: This creates a concentration of 500mcg/ml. So each 1/10 of a ML is 50mcg***8217;s.
Draw the desired amount of IGF in to a syringe. Desired amount should be the approx dosage wanted.
Example- 2mls AA used to reconstitute IGF-1 1mg vial means 5 units on a U100 insulin syringe would equal 25mcg IGF-1 LR3
Pre-load your syringes at 5iu (25mcg IGF-1). Divide your IGF-1 into 40 syringes for storage in the freezer.
Thaw prior to administration. Draw from your NaCL after thawed to buffer (.5ml is enough).
Unknown whether injecting IGF-1 to increase muscle growth is efficacious. Many believe in the value of this powerful growth factor. Question currently is whether IGF-1 is effective when not manufactured by the tissues themselves.
It is possible to go into hypoglycemia fro IGF-1 supplementation. Effect is dose dependant.
IGF-1 (Long R3 IGF-1) Dose:
Light: 25 mcg
Common: 50 mcg
Large: 100 mcg
IGF-1 is administered for one month, give or take a week.
Insulin-like Growth Factor (Long-R3 IGF-1), an 83 amino acid analog of IGF-1 is a highly anabolic hormone released primarily in the liver with the stimulus of growth hormone (HGH).
IGF-1 is the most potent growth factor found in the body and causes muscle cell hyperplasisa.
Freeze dried (lyophilized) IGF-1 (in powder state) should be stored in the freezer (-18 degrees celsius).
Dilute the IGF-1 peptide with 2mls of Acetic Acid (.6%). Assuming (*DO NOT ASSUME*) Acetic Acid (AA) will yield the correct pH balance of your research peptide.
Note: This creates a concentration of 500mcg/ml. So each 1/10 of a ML is 50mcg***8217;s.
Draw the desired amount of IGF in to a syringe. Desired amount should be the approx dosage wanted.
Example- 2mls AA used to reconstitute IGF-1 1mg vial means 5 units on a U100 insulin syringe would equal 25mcg IGF-1 LR3
Pre-load your syringes at 5iu (25mcg IGF-1). Divide your IGF-1 into 40 syringes for storage in the freezer.
Thaw prior to administration. Draw from your NaCL after thawed to buffer (.5ml is enough).
Unknown whether injecting IGF-1 to increase muscle growth is efficacious. Many believe in the value of this powerful growth factor. Question currently is whether IGF-1 is effective when not manufactured by the tissues themselves.
It is possible to go into hypoglycemia fro IGF-1 supplementation. Effect is dose dependant.
vibrant
CHEMICALLY ENGINEERED
Hexarelin
by Anthony Roberts - Hexarelin (HEX) is a peptide GH secretagogue, structurally similar to GHRP-6, in the growth factor family which stimulates the release of growth hormone (GH). It can be used medically to treat GH deficiency.
Background
Although relatively new, Hexarelin is becoming a popular choice as a performance enhancement drug. Hexarelin is currently available from several research companies.
Action
Due to Hexarelin's ability to increase secretion of natural Growth Hormone, most of its effects are similar to those of synthetic GH, although to a slightly lesser extent. Effects of its use include: increase in strength, growth of new muscle fibers, increase in the size of already existing muscle fibers, neural protection, joint rejuvenation, protection and healing. Also, the GH receptors in adipose (fat) tissue allow for potential fat reduction with Hexarelin use. The increase of circulating GH through Hexarelin use causes levels of Insulin-Like Growth Factor (IGF-1) to rise in the liver. IGF-1 is the prime cause of muscle growth in response to GH stimulation.
There is no appetite boost with Hexarelin use (as opposed to GHRP-6***8217;s extreme appetite increase) due to its inability to drastically increase Ghrelin levels that are responsible for added hunger and quicker gastric emptying.
Technical Data
In studies where Hexarelin was injected subcutaneously, Growth Hormone, measured through plasma concentrations, increased significantly and within thirty minutes of injection. GH levels decreased back to normal around four hours post injection (1). The GH increase, has been found to be effective up to 2mg/kg, any further increase in dose was found to be ineffective in causing a GH response (2).
Results showed that Hexarelin's effect on GH stimulation tapered between weeks 4 through 16. Separating cycles by 4 week off periods, avoided the negative feedback loop and the next cycle of Hexarelin produced the same level of results as the first cycle (3).
User Notes
I used Hexarelin awhile back, at a dose of about 200mcg/day, and found it to be very good for healing my injuries, burning a bit of fat, and helped me gain a bit of muscle.
I also have a couple of friends who are powerlifters, and they were able to use Hexarelin to heal an old Pec injury and train pain free while on it. My bodybuilder friends (yes, not only do I have friends, but some are actually bodybuilders) have said that 400 mcg/day of Hexarelin gave them similar results to low doses of GH (maybe 1-2 iu/day would be a good equivalent).
Overall, Hexarelin is a good all purpose anabolic. Also, since we know that IGF and GH use produces a shutdown of your endogenous levels of those hormones, Hexarelin also seems very useful for ***8220;GH-PCT***8221; or ***8220;IGF-PCT***8221;, as it can help restore your natural levels of those hormones after a cycle of them.
References
Imbimbo, B.P., et. al Growth hormone-releasing activity of hexarelin in humans. A dose-response study.Eur J Clin Pharmacol. 1994;46(5):421-5.
Imbimbo, B.P., et. al Growth hormone-releasing activity of hexarelin in humans. A dose-response study.Eur J Clin Pharmacol. 1994;46(5):421-5.
Rahim, A., Shalet, SM Does desensitization to hexarelin occur? Growth Horm IGF Res. 1998 Apr;8 Suppl B:141-3
by Anthony Roberts - Hexarelin (HEX) is a peptide GH secretagogue, structurally similar to GHRP-6, in the growth factor family which stimulates the release of growth hormone (GH). It can be used medically to treat GH deficiency.
Background
Although relatively new, Hexarelin is becoming a popular choice as a performance enhancement drug. Hexarelin is currently available from several research companies.
Action
Due to Hexarelin's ability to increase secretion of natural Growth Hormone, most of its effects are similar to those of synthetic GH, although to a slightly lesser extent. Effects of its use include: increase in strength, growth of new muscle fibers, increase in the size of already existing muscle fibers, neural protection, joint rejuvenation, protection and healing. Also, the GH receptors in adipose (fat) tissue allow for potential fat reduction with Hexarelin use. The increase of circulating GH through Hexarelin use causes levels of Insulin-Like Growth Factor (IGF-1) to rise in the liver. IGF-1 is the prime cause of muscle growth in response to GH stimulation.
There is no appetite boost with Hexarelin use (as opposed to GHRP-6***8217;s extreme appetite increase) due to its inability to drastically increase Ghrelin levels that are responsible for added hunger and quicker gastric emptying.
Technical Data
In studies where Hexarelin was injected subcutaneously, Growth Hormone, measured through plasma concentrations, increased significantly and within thirty minutes of injection. GH levels decreased back to normal around four hours post injection (1). The GH increase, has been found to be effective up to 2mg/kg, any further increase in dose was found to be ineffective in causing a GH response (2).
Results showed that Hexarelin's effect on GH stimulation tapered between weeks 4 through 16. Separating cycles by 4 week off periods, avoided the negative feedback loop and the next cycle of Hexarelin produced the same level of results as the first cycle (3).
User Notes
I used Hexarelin awhile back, at a dose of about 200mcg/day, and found it to be very good for healing my injuries, burning a bit of fat, and helped me gain a bit of muscle.
I also have a couple of friends who are powerlifters, and they were able to use Hexarelin to heal an old Pec injury and train pain free while on it. My bodybuilder friends (yes, not only do I have friends, but some are actually bodybuilders) have said that 400 mcg/day of Hexarelin gave them similar results to low doses of GH (maybe 1-2 iu/day would be a good equivalent).
Overall, Hexarelin is a good all purpose anabolic. Also, since we know that IGF and GH use produces a shutdown of your endogenous levels of those hormones, Hexarelin also seems very useful for ***8220;GH-PCT***8221; or ***8220;IGF-PCT***8221;, as it can help restore your natural levels of those hormones after a cycle of them.
References
Imbimbo, B.P., et. al Growth hormone-releasing activity of hexarelin in humans. A dose-response study.Eur J Clin Pharmacol. 1994;46(5):421-5.
Imbimbo, B.P., et. al Growth hormone-releasing activity of hexarelin in humans. A dose-response study.Eur J Clin Pharmacol. 1994;46(5):421-5.
Rahim, A., Shalet, SM Does desensitization to hexarelin occur? Growth Horm IGF Res. 1998 Apr;8 Suppl B:141-3
vibrant
CHEMICALLY ENGINEERED
Bremelanotide (PT-141)
Bremelanotide PT-141 Dose:
Light: .5mg
Common: 1mg
Large: 2mg
Bremelanotide (PT-141) was developed from Melanotan 2 (MT-II). PT-141 is a metabolite of melanocyte stimulating hormone that targets desire.
Treatment: PT-141 is the only synthetic aphrodisiac. The aphrodisiac effects of Bremelanotide are in a class of its own. Studies have shown Bremelanotide to be effective in treating sexual dysfunction in both men (erectile dysfunction or impotence) and women (sexual arousal disorder). Nine out of ten volunteers experienced sexual arousal in clinical trials. Unlike Viagra and other related medications (PDE5s - blood pushers), PT-141 acts upon the nervous system. Viagra, Cials and Levitra are not considered aphrodisiacs as they do not have any direct effect on the libido. However, treatment with PDE5 inhibitors and PT-141 have known synergy.
Men's Journal Magazine: ...it took hold. I felt a great surge of affection (greater than any regular level of arousal). My body tingled and I developed an erection that wouldn***8217;t quit. For two hours the drug wouldn***8217;t let me out of its grasp ***8212; nor my wife out of mine. -Frederick Kaufman
Females: Women who took part in trials said that they felt a "tingling and a throbbing" along with "a strong desire to have sex." An initial flush occurs post injection, followed by nausea which is dose dependent. For most, effects generally do not take place until a couple hours post injection, peaking around the four hour mark. Men said PT-141 made them feel "younger and more energetic" as well as sexually interested and aroused. "You're ready to take your pants off and go," said user "a drug that makes you not only able to but eager to."
Bremelanotide PT-141 Peptide: Bremelanotide comes in 10mg vials. As a lifestyle peptide, the 10mg product is a lot to consume and may offer up to 20 doses when dosing light. The PT-141 peptide reconstituted with bacteriostatic water remains potent in the fridge for months.
Window of Opportunity: Bremelanotide, injected (subcutaneously), has a unique window of opportunity lasting six to 72 hours. In lab trials female rats exposed to PT-141 began "flirting" with male rats for sex. Postures and movements left no doubt in the male rats minds that they were in the mood. The human PT-141 date is one where the dosage precedes the activity by at least a couple hours. When the stars align, hours after the injection, ...this is your window of opportunity, enjoy.
Mixing: Bacteriostatic water is used for reconstitution.
Example- 1ml(cc) bacteriostatic water per 10mg PT-141 vial equates to a 1mg dose approximately each 10 units on a U100 insulin syringe.
Example- 1ml(cc) bacteriostatic water per 2mg PT-141 vial equates to a 1mg dose approximately every 50 units on a U100 insulin syringe.
Recommended strategy for mixing and dosing would be to reconstitute with the volume that yields a .1ml injection.
Example- 1ml(cc) bacteriostatic water per 10mg PT-141 vial equates to a 1mg dose approximately each 10 units on a U100 insulin syringe.
Example- .2ml(cc) bacteriostatic water per 2mg PT-141 vial equates to a 1mg dose approximately every 10 units on a U100 insulin syringe.
Dosing: Read as much as possible to gain clarity and align expectations. Gradually dosing increases likelihood for success without sides. A test dose of .25-.5mg on the first attempt is recommended. 1mg, give or take a quarter, is the efficacious dose which yields the most positive reports by users.
Bremelanotide PT-141 Dose:
Light: .5mg
Common: 1mg
Large: 2mg
Bremelanotide (PT-141) was developed from Melanotan 2 (MT-II). PT-141 is a metabolite of melanocyte stimulating hormone that targets desire.
Treatment: PT-141 is the only synthetic aphrodisiac. The aphrodisiac effects of Bremelanotide are in a class of its own. Studies have shown Bremelanotide to be effective in treating sexual dysfunction in both men (erectile dysfunction or impotence) and women (sexual arousal disorder). Nine out of ten volunteers experienced sexual arousal in clinical trials. Unlike Viagra and other related medications (PDE5s - blood pushers), PT-141 acts upon the nervous system. Viagra, Cials and Levitra are not considered aphrodisiacs as they do not have any direct effect on the libido. However, treatment with PDE5 inhibitors and PT-141 have known synergy.
Men's Journal Magazine: ...it took hold. I felt a great surge of affection (greater than any regular level of arousal). My body tingled and I developed an erection that wouldn***8217;t quit. For two hours the drug wouldn***8217;t let me out of its grasp ***8212; nor my wife out of mine. -Frederick Kaufman
Females: Women who took part in trials said that they felt a "tingling and a throbbing" along with "a strong desire to have sex." An initial flush occurs post injection, followed by nausea which is dose dependent. For most, effects generally do not take place until a couple hours post injection, peaking around the four hour mark. Men said PT-141 made them feel "younger and more energetic" as well as sexually interested and aroused. "You're ready to take your pants off and go," said user "a drug that makes you not only able to but eager to."
Bremelanotide PT-141 Peptide: Bremelanotide comes in 10mg vials. As a lifestyle peptide, the 10mg product is a lot to consume and may offer up to 20 doses when dosing light. The PT-141 peptide reconstituted with bacteriostatic water remains potent in the fridge for months.
Window of Opportunity: Bremelanotide, injected (subcutaneously), has a unique window of opportunity lasting six to 72 hours. In lab trials female rats exposed to PT-141 began "flirting" with male rats for sex. Postures and movements left no doubt in the male rats minds that they were in the mood. The human PT-141 date is one where the dosage precedes the activity by at least a couple hours. When the stars align, hours after the injection, ...this is your window of opportunity, enjoy.
Mixing: Bacteriostatic water is used for reconstitution.
Example- 1ml(cc) bacteriostatic water per 10mg PT-141 vial equates to a 1mg dose approximately each 10 units on a U100 insulin syringe.
Example- 1ml(cc) bacteriostatic water per 2mg PT-141 vial equates to a 1mg dose approximately every 50 units on a U100 insulin syringe.
Recommended strategy for mixing and dosing would be to reconstitute with the volume that yields a .1ml injection.
Example- 1ml(cc) bacteriostatic water per 10mg PT-141 vial equates to a 1mg dose approximately each 10 units on a U100 insulin syringe.
Example- .2ml(cc) bacteriostatic water per 2mg PT-141 vial equates to a 1mg dose approximately every 10 units on a U100 insulin syringe.
Dosing: Read as much as possible to gain clarity and align expectations. Gradually dosing increases likelihood for success without sides. A test dose of .25-.5mg on the first attempt is recommended. 1mg, give or take a quarter, is the efficacious dose which yields the most positive reports by users.
vibrant
CHEMICALLY ENGINEERED
Melanotan One (MT-1)
Afamelanotide (M-I) Dose:
Light: .5mg
Common: 1mg
Large: 2mg Melanotan/Afamelanotide synthetic melanocyte stimulating hormone (a-MSH) induces skin pigmentation through melanogenisis, melanin production. Melanin prevents cellular damage in the skin by absorbing, reflecting and refracting light. Melanotan reduces sun damage to UV exposed skin transforming cells to produce dark protective melanin.
Melanotan Results: Melanotan favors production of eumelanin (black/brown) over pheomelanin pigment. Injecting this linear amino acid Melanotan 1 peptide offers super-physiological levels of tanning ability.
Research Use: The half-life of Melanotan peptides is very brief. Afamelanotide is being developed in implant form for the ease of use in dermatology. The implant contains a controlled release effecting melanin density for months. Melanotan One is offered in research peptide form (Melanotan).
Lifestyle: Melanocortins have the potential to be the next big thing in lifestyle cosmetic treatment (Viagra, Botox, etc). Melanotan can be appropriately used continuously as well as intermittently.
Recommended Therapy: Intermittent therapy, lasting 10 days (skin type III) to 6 months (skin type I) works well. Take note how long after your Melanotan administration melanin density stays elevated.
Peptide Molecule: Two amino acids present in the bodies natural a-MSH have been changed in production of Melanotan 1 increasing stablity. Melanotan only works when injected subcutaneously.
Amino acid sequence: Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2
Clinical Trial: Melanotan is still undergoing clinical trials and has not reached approved status. People use on the pretenses and understanding that it is for research purposes only. Users may suffer from slight nausea and flushing after subcutaneous injection; however it is reported to be mild and pass quickly.
Administration of Research Melanotan
Safe and controlled administration of Afamelanotide for research is done much like that of Melanotan 2. Melanotan One offered as a peptide in a multi-dose sterile vial is desirable. Implants, nasal sprays and pills are not applicable/efficacious at the present time.
Melanotan One is less efficacious than its counterpart Melanotan 2 for achieving a dark tan. Afamelanotide will therefore require 8-10x the dosage to see comparable results. Melanotan One users want minimum side and peripheral effects with a focus on photoprotection. Be patient and prepared through your Melanotan journey.
Melanotan Treatment: Dosing According to Skin Type
Fitzpatrick Skin Type I: 1mg-2mg/day. 100mg total may be necessary to achieve desired color. UV exposure after at least 20mg in system
Fitzpatrick Skin Type II: .75mg-1.5mg/day. 60mg should be sufficient to get color. UV exposure after 10-20mg
Fitzpatrick Skin Type III: .5mg-1mg/day. A sunless tan may be realistic
Fitzpatrick Skin Type IV: Do not use Melanotan
Melanotan Video from Australia
Melanotan can assist the develop a protective tan in users. A natural tan is developed in response to cell damage caused by UV radiation. Ultraviolet rays penetrate the upper layers of the skin, triggering a-MSH, stimulating melanin production. Melanin deposits act as a natural sunblock at the cellular level. Melanotan tanning injections may offer a way to bring upon a safe, cosmetic tan with less damage.
Afamelanotide (M-I) Dose:
Light: .5mg
Common: 1mg
Large: 2mg Melanotan/Afamelanotide synthetic melanocyte stimulating hormone (a-MSH) induces skin pigmentation through melanogenisis, melanin production. Melanin prevents cellular damage in the skin by absorbing, reflecting and refracting light. Melanotan reduces sun damage to UV exposed skin transforming cells to produce dark protective melanin.
Melanotan Results: Melanotan favors production of eumelanin (black/brown) over pheomelanin pigment. Injecting this linear amino acid Melanotan 1 peptide offers super-physiological levels of tanning ability.
Research Use: The half-life of Melanotan peptides is very brief. Afamelanotide is being developed in implant form for the ease of use in dermatology. The implant contains a controlled release effecting melanin density for months. Melanotan One is offered in research peptide form (Melanotan).
Lifestyle: Melanocortins have the potential to be the next big thing in lifestyle cosmetic treatment (Viagra, Botox, etc). Melanotan can be appropriately used continuously as well as intermittently.
Recommended Therapy: Intermittent therapy, lasting 10 days (skin type III) to 6 months (skin type I) works well. Take note how long after your Melanotan administration melanin density stays elevated.
Peptide Molecule: Two amino acids present in the bodies natural a-MSH have been changed in production of Melanotan 1 increasing stablity. Melanotan only works when injected subcutaneously.
Amino acid sequence: Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2
Clinical Trial: Melanotan is still undergoing clinical trials and has not reached approved status. People use on the pretenses and understanding that it is for research purposes only. Users may suffer from slight nausea and flushing after subcutaneous injection; however it is reported to be mild and pass quickly.
Administration of Research Melanotan
Safe and controlled administration of Afamelanotide for research is done much like that of Melanotan 2. Melanotan One offered as a peptide in a multi-dose sterile vial is desirable. Implants, nasal sprays and pills are not applicable/efficacious at the present time.
Melanotan One is less efficacious than its counterpart Melanotan 2 for achieving a dark tan. Afamelanotide will therefore require 8-10x the dosage to see comparable results. Melanotan One users want minimum side and peripheral effects with a focus on photoprotection. Be patient and prepared through your Melanotan journey.
Melanotan Treatment: Dosing According to Skin Type
Fitzpatrick Skin Type I: 1mg-2mg/day. 100mg total may be necessary to achieve desired color. UV exposure after at least 20mg in system
Fitzpatrick Skin Type II: .75mg-1.5mg/day. 60mg should be sufficient to get color. UV exposure after 10-20mg
Fitzpatrick Skin Type III: .5mg-1mg/day. A sunless tan may be realistic
Fitzpatrick Skin Type IV: Do not use Melanotan
Melanotan Video from Australia
Melanotan can assist the develop a protective tan in users. A natural tan is developed in response to cell damage caused by UV radiation. Ultraviolet rays penetrate the upper layers of the skin, triggering a-MSH, stimulating melanin production. Melanin deposits act as a natural sunblock at the cellular level. Melanotan tanning injections may offer a way to bring upon a safe, cosmetic tan with less damage.
vibrant
CHEMICALLY ENGINEERED
Melanotan II Dose:
Low: 250 mcg
Moderate: 500 mcg
Large: 1mg
Melanotan II analog of alpha-melanocyte stimulating hormone (a-MSH). Melanotan peptides are safe and efficacious with growing long term data. Melanotan 2 is a freeze dried peptide sealed in a sterile multi-use vial. Generic 10mg Melanotan II peptide with green plastic flip top:
Melanotan injections act on melanocytes to stimulate melanin production in the skin. Melanin is the body's pigment responsible for a photoprotective safe tan.
Sunless tanning peptides begin with the sequence: His-Phe-Arg-Trp. Melanotan tanning peptide binds to melanocortin receptors influencing pigmentation, inflammation, energy, appetite and sexual function. Melanotan 2 has a small protective amino acid structure that show effect at the melanocortin 1, 3, 4 and 5 receptors.
Melanotan 2 is a small efficient molecule as compared to the linear Melanotan I design after natural melanocyte stimulating hormone peptide. Melanotan 2 passes the blood brain barrier (BBB) stimulating the aphrodisiac and weight loss effects through the melanocortin system. Melanotan is approximately 1,000 times more potent than natural a-MSH.
Fair skinned folks who never tan, always burn in the sun, can achieve a natural tan when using Melanotan 2. For people with sun allergies/mutated receptors, synthetic melanotropin peptide supplements are life changing. A natural tan developed over time is the best defense against skin cancer, to which the fair skin can now acheive. MT-2 was designed to reduce skin cancer rates and potentially for effective sunless tanning.
Athletes and fitness enthusiasts use Melanotan for accelerated tanning, libido increase and appetite suppression. MT-2 was dubbed the Barbie drug and has been highlighted in wired magazine. Synthetic melanocortin use helps attain a tan with the least amount of exposure to harmful ultraviolet radiation. Melanotan II continues to be the most effective tanning peptide sold online.
Fitzpatrick skin type: Skin type I and II, the lower of the skin types on the Fitzpatrick scale are the best candidates for Melanotan
Treatment: Melanotan stimulates melanin, particularly low skin types
Disclaimer: Please pursue information regarding the usage of these products from your own research, academic journals, or the research of your in-house scientific team. Products sold for research purposes are not for human consumption.
Melanotan 2 Peptide: Melanotan 2 peptides come in 5mg and 10mg sizes. Photograph at left shows a 5mg and 10mg MT-2 peptide as an example. Peptides within photograph were synthesized by the same laboratory, contain no filler and therefore volume reflects content. All peptides and freeze drying processes are not created equal. Current MT-2 industry standard is the 10mg, 2ml vial size.
Reconstituted with bacteriostatic water, MT-2 peptide remains potent and preserved. Reconstituting (mixing) your Melanotan 2 peptide is a necessity and will require proper due diligence for results. Nasal sprays, pre-mixed Melanotan 2, pills, oral and loose powder are less than legitimate. Enzymes will render the peptide inactive if ingested. Purchase only pure Melanotan II.
Shipping and Handling: Melanotan peptides are durable and stable. Shipping in the summer not a problem for tanning injections. When receiving MT-2 it is recommended to store in the refrigerator.
Mixing Melanotan: 1ml Bacteriostatic water reconstitutes and preserves tanning peptide Melanotan II. Dilute with more volume for improved dosing accuracy (micrograms).
Remove plastic flip top from vial to expose rubber stopper. Needle will pierce the stopper making way inside the vial to turn the white powder into a clear liquid.
Calculator: Add 100 units (1ml) of water to the vial. 1ml Bacteriostatic water will minimize injection volume and simplify arithmetic. Dosing measurements are often mentioned in both milligram (mg) and microgram (mcg).
Research Peptide Calculator
1ml syringe (U100), 1ml Bact Water to Reconstitute
Calculations for .5mg or 500mcg dose:
Step 1= 1ml
Step 2= 10mg MT-II
Step 3= 1ml bact water
Step 4= 500mcg dose
5 units on your insulin syringe (approximately 1/20th of a U100 syringe)
Needles: 29-31 gauge X 1/2", 1 CC (100 unit). That is a typical insulin needle used to mix as well as inject. Use needles one time only. Once your technique perfected, injections are almost painless. Smaller 1/2 and 1/3cc syringes offer greater measurement accuracy and pre-loading convenience.
Melanotan II Dose: Your first injection should be a very small dose, for example .25mg (250mcg). See how you react. Goal should be to feel nothing. Dose after dinner, before bed. Any dosing chart stating that you should take a high dose (according to your weight) is dated and potentially dangerous.
Loading dose: Load with .5-1mg once a day. People who have used doses in this range generally report getting excellent results. Don’t worry if you miss occasional days. It will not make much difference, focus on the cumulative effects. A tan generally sets in 3 days after UV rays. Dose and expose yourself gradually to UVR when tanning.
Maintenance dose: Maintenance is taking doses less frequently than daily to avoid becoming darker than you want. Yes, that will happen. With enough UVR, you will get much darker than you have even been before. A maintenance dose can help prolong super-physiological photo-protection MT-2 delivers.
UV Radiation: Melanotan is a poor sunless tanner. UV (from sun or a tanning bed) light is necessary to develop a tan for most folks. Without it, almost nothing happens. In other words, NO UV = NO TAN. Melanotan use for a full month and with UV exposure, you (and your friends) will be astounded by how fast and how dark MT-II tanning results. Areas of skin that are typically sun-exposed in your day to day life will respond more readily to the effects of the melanotan peptides, take photo therapy serious with Melanotan II.
Melanotan 2 Weight Loss: Melanotan II peptide usage results in adipocyte lipolysis. Dose low-moderate between meals to increase fatty acid oxidation, reduce food intake, and increase energy.
Do you have to inject MT-II?
Yes. The best, most efficient method of administering Melanotan peptides are subcutaneous (subq) injections. Nasal sprays are inconsistent and inefficient. No detectable levels were observed following oral dosing - pills do not work.
Note: There are many things you will need to consider before experimenting with this peptide. Cyclic analogues (MT-II) have a wide range of peripheral effects and systemic control is always going to pose an issue in clinical use. Needless to say, MT-II is not an approved or regulated product. MT-II is legal to buy, possess, etc. Variables such as skin type and individual goals need assessment. Ask for critiques, plans and create a user log during use. Seasoned users are generally more than happy to offer help on how to take peptides.
When supplementing a-MSH (Melanotan II) to tan keep in mind that tanning is literally a side effect. The tanning response is, in reality, a physiological repair mechanism to UV damage of the skin cells (epidermis/dermis). Melanocyte stimulating hormone is not going to color your skin, it is going to make your own skin create its own tan and that in turn creates protection. If you are looking to be some bronzed beach God with perfectly uniform and specific color then you are better off to going to mystic tan. Redheads, for example, naturally produce a variant form of melanin that is yellowish-red (pheomelanin). Do not expect a black tan on ginger skin without serious diligence.
Melanotan Dosing according to Skin Type: Knowing your skin type is one detail which will help create a public user log. There are 10s of thousands of melanotan users worldwide who share the experience. Raise awareness and help others who want to hear success stories, complications and failures.
Am I a good candidate for MT-II?
Melanotan is best suited for the folks with skin types I & II. Prior sun damage, scars, tattoos, freckles, moles, hair color, etc are deciding factors prospective MT-2 users consider.
How should I dose MT-II?
Melanotan II dosage it is recommended to start out small and build up. A typical starting dose is around .25mg and max dose reaching 1mg. Desensitization happens quick, the first administration is an opportunity to dose low to avoid Melanotan 2 side effects. Same goes for bremelanotide (PT-141) dosage unfortunately.
Melanotan Instructions: There is no magic pill or formula. Instructions do not exist for research peptides. Few dermatologists are familiar with Melanotan. The skin is a large, unpredictable organ. Feel comfortable and confident with MT-II before use. Check out as many before and after photos and user logs as you can. A skin type I individual may have to commit months of dedication before dialing in their desired results, be patient and ask questions.
How much MT-II should I buy and how long will it last?
Skin type I: 30-50mg
Skin type II: 20-30mg
Skin type III: 10mg
Should last entire summer or season
How soon will I begin to see Melanotan II results?
Change in skin tone after 2-3 weeks should be anticipated. If you have freckles, expect them to get darker before your actual skin color changes. Brace yourself.
How long will the tan last?
A tan developed using Melanotan 2 lasts much longer than an ordinary tan. A well-tanned person returning from a beach holiday will lose most of the tan in a month if they stop getting sun. But if they had been using Melanotan 2 and continued on maintenance after returning, they would still have most of their tan 3 months later.
Side effects of Melanotan II?
Possible short-term side effects include: nausea, appetite loss, facial flushing and increased libido. Melanotan II side effects may be noticeable during the first few days of treatment but should taper off as the body desensitizes.
Low: 250 mcg
Moderate: 500 mcg
Large: 1mg
Melanotan II analog of alpha-melanocyte stimulating hormone (a-MSH). Melanotan peptides are safe and efficacious with growing long term data. Melanotan 2 is a freeze dried peptide sealed in a sterile multi-use vial. Generic 10mg Melanotan II peptide with green plastic flip top:
Melanotan injections act on melanocytes to stimulate melanin production in the skin. Melanin is the body's pigment responsible for a photoprotective safe tan.
Sunless tanning peptides begin with the sequence: His-Phe-Arg-Trp. Melanotan tanning peptide binds to melanocortin receptors influencing pigmentation, inflammation, energy, appetite and sexual function. Melanotan 2 has a small protective amino acid structure that show effect at the melanocortin 1, 3, 4 and 5 receptors.
Melanotan 2 is a small efficient molecule as compared to the linear Melanotan I design after natural melanocyte stimulating hormone peptide. Melanotan 2 passes the blood brain barrier (BBB) stimulating the aphrodisiac and weight loss effects through the melanocortin system. Melanotan is approximately 1,000 times more potent than natural a-MSH.
Fair skinned folks who never tan, always burn in the sun, can achieve a natural tan when using Melanotan 2. For people with sun allergies/mutated receptors, synthetic melanotropin peptide supplements are life changing. A natural tan developed over time is the best defense against skin cancer, to which the fair skin can now acheive. MT-2 was designed to reduce skin cancer rates and potentially for effective sunless tanning.
Athletes and fitness enthusiasts use Melanotan for accelerated tanning, libido increase and appetite suppression. MT-2 was dubbed the Barbie drug and has been highlighted in wired magazine. Synthetic melanocortin use helps attain a tan with the least amount of exposure to harmful ultraviolet radiation. Melanotan II continues to be the most effective tanning peptide sold online.
Fitzpatrick skin type: Skin type I and II, the lower of the skin types on the Fitzpatrick scale are the best candidates for Melanotan
Treatment: Melanotan stimulates melanin, particularly low skin types
Disclaimer: Please pursue information regarding the usage of these products from your own research, academic journals, or the research of your in-house scientific team. Products sold for research purposes are not for human consumption.
Melanotan 2 Peptide: Melanotan 2 peptides come in 5mg and 10mg sizes. Photograph at left shows a 5mg and 10mg MT-2 peptide as an example. Peptides within photograph were synthesized by the same laboratory, contain no filler and therefore volume reflects content. All peptides and freeze drying processes are not created equal. Current MT-2 industry standard is the 10mg, 2ml vial size.
Reconstituted with bacteriostatic water, MT-2 peptide remains potent and preserved. Reconstituting (mixing) your Melanotan 2 peptide is a necessity and will require proper due diligence for results. Nasal sprays, pre-mixed Melanotan 2, pills, oral and loose powder are less than legitimate. Enzymes will render the peptide inactive if ingested. Purchase only pure Melanotan II.
Shipping and Handling: Melanotan peptides are durable and stable. Shipping in the summer not a problem for tanning injections. When receiving MT-2 it is recommended to store in the refrigerator.
Mixing Melanotan: 1ml Bacteriostatic water reconstitutes and preserves tanning peptide Melanotan II. Dilute with more volume for improved dosing accuracy (micrograms).
Remove plastic flip top from vial to expose rubber stopper. Needle will pierce the stopper making way inside the vial to turn the white powder into a clear liquid.
Calculator: Add 100 units (1ml) of water to the vial. 1ml Bacteriostatic water will minimize injection volume and simplify arithmetic. Dosing measurements are often mentioned in both milligram (mg) and microgram (mcg).
Research Peptide Calculator
1ml syringe (U100), 1ml Bact Water to Reconstitute
Calculations for .5mg or 500mcg dose:
Step 1= 1ml
Step 2= 10mg MT-II
Step 3= 1ml bact water
Step 4= 500mcg dose
5 units on your insulin syringe (approximately 1/20th of a U100 syringe)
Needles: 29-31 gauge X 1/2", 1 CC (100 unit). That is a typical insulin needle used to mix as well as inject. Use needles one time only. Once your technique perfected, injections are almost painless. Smaller 1/2 and 1/3cc syringes offer greater measurement accuracy and pre-loading convenience.
Melanotan II Dose: Your first injection should be a very small dose, for example .25mg (250mcg). See how you react. Goal should be to feel nothing. Dose after dinner, before bed. Any dosing chart stating that you should take a high dose (according to your weight) is dated and potentially dangerous.
Loading dose: Load with .5-1mg once a day. People who have used doses in this range generally report getting excellent results. Don’t worry if you miss occasional days. It will not make much difference, focus on the cumulative effects. A tan generally sets in 3 days after UV rays. Dose and expose yourself gradually to UVR when tanning.
Maintenance dose: Maintenance is taking doses less frequently than daily to avoid becoming darker than you want. Yes, that will happen. With enough UVR, you will get much darker than you have even been before. A maintenance dose can help prolong super-physiological photo-protection MT-2 delivers.
UV Radiation: Melanotan is a poor sunless tanner. UV (from sun or a tanning bed) light is necessary to develop a tan for most folks. Without it, almost nothing happens. In other words, NO UV = NO TAN. Melanotan use for a full month and with UV exposure, you (and your friends) will be astounded by how fast and how dark MT-II tanning results. Areas of skin that are typically sun-exposed in your day to day life will respond more readily to the effects of the melanotan peptides, take photo therapy serious with Melanotan II.
Melanotan 2 Weight Loss: Melanotan II peptide usage results in adipocyte lipolysis. Dose low-moderate between meals to increase fatty acid oxidation, reduce food intake, and increase energy.
Do you have to inject MT-II?
Yes. The best, most efficient method of administering Melanotan peptides are subcutaneous (subq) injections. Nasal sprays are inconsistent and inefficient. No detectable levels were observed following oral dosing - pills do not work.
Note: There are many things you will need to consider before experimenting with this peptide. Cyclic analogues (MT-II) have a wide range of peripheral effects and systemic control is always going to pose an issue in clinical use. Needless to say, MT-II is not an approved or regulated product. MT-II is legal to buy, possess, etc. Variables such as skin type and individual goals need assessment. Ask for critiques, plans and create a user log during use. Seasoned users are generally more than happy to offer help on how to take peptides.
When supplementing a-MSH (Melanotan II) to tan keep in mind that tanning is literally a side effect. The tanning response is, in reality, a physiological repair mechanism to UV damage of the skin cells (epidermis/dermis). Melanocyte stimulating hormone is not going to color your skin, it is going to make your own skin create its own tan and that in turn creates protection. If you are looking to be some bronzed beach God with perfectly uniform and specific color then you are better off to going to mystic tan. Redheads, for example, naturally produce a variant form of melanin that is yellowish-red (pheomelanin). Do not expect a black tan on ginger skin without serious diligence.
Melanotan Dosing according to Skin Type: Knowing your skin type is one detail which will help create a public user log. There are 10s of thousands of melanotan users worldwide who share the experience. Raise awareness and help others who want to hear success stories, complications and failures.
Am I a good candidate for MT-II?
Melanotan is best suited for the folks with skin types I & II. Prior sun damage, scars, tattoos, freckles, moles, hair color, etc are deciding factors prospective MT-2 users consider.
How should I dose MT-II?
Melanotan II dosage it is recommended to start out small and build up. A typical starting dose is around .25mg and max dose reaching 1mg. Desensitization happens quick, the first administration is an opportunity to dose low to avoid Melanotan 2 side effects. Same goes for bremelanotide (PT-141) dosage unfortunately.
Melanotan Instructions: There is no magic pill or formula. Instructions do not exist for research peptides. Few dermatologists are familiar with Melanotan. The skin is a large, unpredictable organ. Feel comfortable and confident with MT-II before use. Check out as many before and after photos and user logs as you can. A skin type I individual may have to commit months of dedication before dialing in their desired results, be patient and ask questions.
How much MT-II should I buy and how long will it last?
Skin type I: 30-50mg
Skin type II: 20-30mg
Skin type III: 10mg
Should last entire summer or season
How soon will I begin to see Melanotan II results?
Change in skin tone after 2-3 weeks should be anticipated. If you have freckles, expect them to get darker before your actual skin color changes. Brace yourself.
How long will the tan last?
A tan developed using Melanotan 2 lasts much longer than an ordinary tan. A well-tanned person returning from a beach holiday will lose most of the tan in a month if they stop getting sun. But if they had been using Melanotan 2 and continued on maintenance after returning, they would still have most of their tan 3 months later.
Side effects of Melanotan II?
Possible short-term side effects include: nausea, appetite loss, facial flushing and increased libido. Melanotan II side effects may be noticeable during the first few days of treatment but should taper off as the body desensitizes.
vibrant
CHEMICALLY ENGINEERED
Mechano Growth Factor
You want to GROW?
When Human Growth Hormone (GH) was first introduced to the bodybuilding world, everyone had high hopes. Those hopes fizzled out pretty quickly, as bodybuilders experimented with absurdly low dosages (2iu/every other day), necessitated by its high cost. As GH costs fell due to more efficient manufacturing processes (i.e. it was no longer being extracted from cadavers), bodybuilders were able to use more of it, and subsequently began to see better results. We saw the same phenomenon with the anabolic mediator of GH, Insulin-like Growth Factor-1, and later with its analogue, LR3IGF-1.
Now, we***8217;ve seen the emergence of yet another compound further down the hormonal cascade: Mechano Growth Factor (MGH). As you probably know, skeletal muscle responds to resistance training (or any mechanical overload), by increasing its size (hopefully). If you ***8216;detrain***8217; that muscle (i.e. don***8217;t use it regularly), it atrophies and gets smaller.
Similarly, when you are in your teens and early twenties GH and IGF-1 levels are high, and as you age, those levels are lowered naturally. And if you***8217;ve been playing along at home, you***8217;re probably figuring out that GH and IGF-1 are pieces of the hormonal puzzle that result in this muscle growth (or loss). These growth factors are produced in the liver and other areas, but also in skeletal tissue in response to training induced damage. Now, pay attention, because this is the important part - growth factors produced within the muscle as a response to resistance training likely play a major role in repair, adaptation, hypertrophy (muscle growth), and also ageing.
Scientists have discovered that many of GH***8217;s anabolic and regenerative effects are actually mediated by insulin like growth factor 1. Thus, the next logical step for bodybuilders (if bodybuilders can be said to follow some kind of logic), was to start experimenting with IGF-1 and later with the more potent version, LR3IGF-1.
The thing is, we now know that IGF-1 actually exists in the body in multiple isoforms. The isoform that seems most useful to us, differs slightly from that which is produced in the liver (IGF-1Ea). It also appears to be the significantly more anabolic of the two we***8217;re looking at here (i.e. that which is produced in the liver vs. that which is produced in the muscle). This is because it is hyper-sensitive to the signals produced by local muscular damage induced by resistance training. This more anabolic isoform of IGF-1 is called ***8220;IGF-1Ec***8221; or mechano growth factor (MGF).
That***8217;s right, MGF, the mysterious hormone that seems to be only whispered in e-mails and PMs on the net, is actually just another variant of IGF-1. Yeah, if you***8217;ve used IGF-1 or even GH, then technically, you***8217;ve already been taking advantage of MGF. In fact, if you work out with weights, you***8217;ve been producing your own MGF - as this particular isoform of IGF-1 is only detected in normal muscle after mechanical stimulation (such as resistance training). Remember, MGF is just a name for the particular type of IGF-1 which is produced locally in the muscle as part of the anabolic repair response to resistance training.
Here***8217;s how it happens***8230;
When we workout with weights, the IGF-1 gene is differentially spliced during the body***8217;s response to local muscular overload. First it is spliced to produce predominantly IGF-1Ec (called the MGF splice variant of IGF-1). This initial splicing appears to stimulate satellite cells into activation. This in turn allows the activation of extra undamaged nuclei required for muscle fiber growth and repair to occur. In addition, the appearance of MGF initiates the upregulation of new protein synthesis. After this initial and short lived burst of splicing, IGF-1 production switches towards producing a systemic release of IGF-1Ea from the liver, which upregulates protein synthesis as well, but over a longer time line. This secondary release of IGF-1Ea noticeably less anabolic than the initial release of IGF-1Ec (MGF).
It is the expression of the various IGF-1 splice variants, over the course of the healing and regrowth phase of muscle repair, that is responsible for a generous portion of the body***8217;s ability to engender growth in target tissue (which is, of course, skeletal muscle). It would appear that the introduction of this hormone, whether by weight training or by injection, will cause a response in the area resulting in localized muscle growth.
But, in the end, we***8217;re still just talking about IGF-1, just a particular form of it***8230;
As is often the case with the ***8216;hot new drug on the net***8217;, the rabbit was always in the hat, and the magic was only a trick. MGF is simply a variant of something we***8217;ve had around for over a decade. It***8217;s just not as sexy when we call it ***8220;IGF-1Ec***8221;, but regardless of what we call it, it***8217;s still just an isoform of IGF-1. In fact, the anabolic actions of both IGF-1 as well as MGF are achieved by stimulating and upregulating protein synthesis, and proliferating growth and activation of satellite cells. Actually, this latter function of MGF is quite important, as satellite cells are the mononucleated cells in muscle fibers located between the sarcolemma and the basal lamina. Proliferation and activation of these cells results in the creation of new muscle.
And all of this leads us to the real question here, which is: ***8220;How effective is this stuff?***8221;
Well, most of what we have to go on presently is studies in the elderly (which there are very few of), and studies in rodents. The most relevant rodent data has been shown that MGF is a very potent inducer of muscle growth when it***8217;s introduced into the muscle via an intramuscular injection. In fact, in one study MGF caused a 20% increase in the weight of the injected muscle within 2 weeks! Further investigation elucidated that this was actually due to an increase in the size of the muscle fibers!
However, scientists are coming around to identifying the one-two-punch of MGF with regards to both inducing satellite cell activation as well as protein synthesis as clearly showing an advantage over other types of (systemic, or liver derived) IGF-1. In fact, when locally produced IGF-1 was compared to systemic IGF-1 (i.e. IGF-1Ea vs. IGF-1Ec) in later rodent studies, the superiority of the locally produced IGF-1 variants (MGF) were clearly elucidated.
It may just be that overexpression of MGF (IGF-1Ec) and the subsequent overexpression of IGF-1Ea are the deciding factors in whether a muscle will grow or not. But remember what I told you at the beginning about GH and IGF-1 in general? Until the prices on MGF go down to affordable levels, bodybuilders are probably going to be using substandard doses of MGF and reporting substandard results; or using tiny amounts with boatloads of other pharmaceuticals, and claiming absurd results. In the end, what we***8217;re looking at is another variant of IGF-1, that***8217;s probably going to be even better than LR3IGF-1 at producing muscle growth - once somebody finds a way to produce it at affordable prices.
Sincerely,
Anthony Roberts
You want to GROW?
When Human Growth Hormone (GH) was first introduced to the bodybuilding world, everyone had high hopes. Those hopes fizzled out pretty quickly, as bodybuilders experimented with absurdly low dosages (2iu/every other day), necessitated by its high cost. As GH costs fell due to more efficient manufacturing processes (i.e. it was no longer being extracted from cadavers), bodybuilders were able to use more of it, and subsequently began to see better results. We saw the same phenomenon with the anabolic mediator of GH, Insulin-like Growth Factor-1, and later with its analogue, LR3IGF-1.
Now, we***8217;ve seen the emergence of yet another compound further down the hormonal cascade: Mechano Growth Factor (MGH). As you probably know, skeletal muscle responds to resistance training (or any mechanical overload), by increasing its size (hopefully). If you ***8216;detrain***8217; that muscle (i.e. don***8217;t use it regularly), it atrophies and gets smaller.
Similarly, when you are in your teens and early twenties GH and IGF-1 levels are high, and as you age, those levels are lowered naturally. And if you***8217;ve been playing along at home, you***8217;re probably figuring out that GH and IGF-1 are pieces of the hormonal puzzle that result in this muscle growth (or loss). These growth factors are produced in the liver and other areas, but also in skeletal tissue in response to training induced damage. Now, pay attention, because this is the important part - growth factors produced within the muscle as a response to resistance training likely play a major role in repair, adaptation, hypertrophy (muscle growth), and also ageing.
Scientists have discovered that many of GH***8217;s anabolic and regenerative effects are actually mediated by insulin like growth factor 1. Thus, the next logical step for bodybuilders (if bodybuilders can be said to follow some kind of logic), was to start experimenting with IGF-1 and later with the more potent version, LR3IGF-1.
The thing is, we now know that IGF-1 actually exists in the body in multiple isoforms. The isoform that seems most useful to us, differs slightly from that which is produced in the liver (IGF-1Ea). It also appears to be the significantly more anabolic of the two we***8217;re looking at here (i.e. that which is produced in the liver vs. that which is produced in the muscle). This is because it is hyper-sensitive to the signals produced by local muscular damage induced by resistance training. This more anabolic isoform of IGF-1 is called ***8220;IGF-1Ec***8221; or mechano growth factor (MGF).
That***8217;s right, MGF, the mysterious hormone that seems to be only whispered in e-mails and PMs on the net, is actually just another variant of IGF-1. Yeah, if you***8217;ve used IGF-1 or even GH, then technically, you***8217;ve already been taking advantage of MGF. In fact, if you work out with weights, you***8217;ve been producing your own MGF - as this particular isoform of IGF-1 is only detected in normal muscle after mechanical stimulation (such as resistance training). Remember, MGF is just a name for the particular type of IGF-1 which is produced locally in the muscle as part of the anabolic repair response to resistance training.
Here***8217;s how it happens***8230;
When we workout with weights, the IGF-1 gene is differentially spliced during the body***8217;s response to local muscular overload. First it is spliced to produce predominantly IGF-1Ec (called the MGF splice variant of IGF-1). This initial splicing appears to stimulate satellite cells into activation. This in turn allows the activation of extra undamaged nuclei required for muscle fiber growth and repair to occur. In addition, the appearance of MGF initiates the upregulation of new protein synthesis. After this initial and short lived burst of splicing, IGF-1 production switches towards producing a systemic release of IGF-1Ea from the liver, which upregulates protein synthesis as well, but over a longer time line. This secondary release of IGF-1Ea noticeably less anabolic than the initial release of IGF-1Ec (MGF).
It is the expression of the various IGF-1 splice variants, over the course of the healing and regrowth phase of muscle repair, that is responsible for a generous portion of the body***8217;s ability to engender growth in target tissue (which is, of course, skeletal muscle). It would appear that the introduction of this hormone, whether by weight training or by injection, will cause a response in the area resulting in localized muscle growth.
But, in the end, we***8217;re still just talking about IGF-1, just a particular form of it***8230;
As is often the case with the ***8216;hot new drug on the net***8217;, the rabbit was always in the hat, and the magic was only a trick. MGF is simply a variant of something we***8217;ve had around for over a decade. It***8217;s just not as sexy when we call it ***8220;IGF-1Ec***8221;, but regardless of what we call it, it***8217;s still just an isoform of IGF-1. In fact, the anabolic actions of both IGF-1 as well as MGF are achieved by stimulating and upregulating protein synthesis, and proliferating growth and activation of satellite cells. Actually, this latter function of MGF is quite important, as satellite cells are the mononucleated cells in muscle fibers located between the sarcolemma and the basal lamina. Proliferation and activation of these cells results in the creation of new muscle.
And all of this leads us to the real question here, which is: ***8220;How effective is this stuff?***8221;
Well, most of what we have to go on presently is studies in the elderly (which there are very few of), and studies in rodents. The most relevant rodent data has been shown that MGF is a very potent inducer of muscle growth when it***8217;s introduced into the muscle via an intramuscular injection. In fact, in one study MGF caused a 20% increase in the weight of the injected muscle within 2 weeks! Further investigation elucidated that this was actually due to an increase in the size of the muscle fibers!
However, scientists are coming around to identifying the one-two-punch of MGF with regards to both inducing satellite cell activation as well as protein synthesis as clearly showing an advantage over other types of (systemic, or liver derived) IGF-1. In fact, when locally produced IGF-1 was compared to systemic IGF-1 (i.e. IGF-1Ea vs. IGF-1Ec) in later rodent studies, the superiority of the locally produced IGF-1 variants (MGF) were clearly elucidated.
It may just be that overexpression of MGF (IGF-1Ec) and the subsequent overexpression of IGF-1Ea are the deciding factors in whether a muscle will grow or not. But remember what I told you at the beginning about GH and IGF-1 in general? Until the prices on MGF go down to affordable levels, bodybuilders are probably going to be using substandard doses of MGF and reporting substandard results; or using tiny amounts with boatloads of other pharmaceuticals, and claiming absurd results. In the end, what we***8217;re looking at is another variant of IGF-1, that***8217;s probably going to be even better than LR3IGF-1 at producing muscle growth - once somebody finds a way to produce it at affordable prices.
Sincerely,
Anthony Roberts
vibrant
CHEMICALLY ENGINEERED
PEG-MGF (PEGylated Mechano Growth Factor)
MGF is a splice variant of the IGF gene which increases stem cell count in the muscle and allows for muscle fibers to fuse and mature. This is a process required for growth of adult muscle. Natural MGF is made locally and does not travel into the bloodstream. Synthetic MGF is water based and when administered intramuscularly, travels into the bloodstream. MGF is only stable in the blood stream for only a few minutes.
Multiple medical studies have verified the swiftly enhanced muscle growth, rapid recovery from intense training, and incredible fat loss properties of the remarkably fast-acting Pituitary Growth Hormone formula. Order today and start seeing incredible improvement in your general health and overall well-being!
PEGylation is the act of attaching a Polyethylene glycol (PEG) structure to another larger molecule (in this case, MGF). The PEG acts as a protective coating and the theory here is that this will allow the MGF to be carried through the blood stream without being broken down.
Background
I have to be honest here, and say that in my estimation, PEGylating MGF is basically something a research chemical company did to have a bit of a market with no competition for awhile. That***8217;s not to say that it***8217;s not a decent product, but honestly, in this particular case, I feel that marketing was in the drivers seat with the development of this version of MGF, and science was in the backseat asking ***8220;are we there yet?***8221;.
Action
MGF is produced biologically when muscle fibers are broken down through resistance (weight training). It is a potent factor in muscle growth. MGF stimulates muscle growth, creates new muscle fibers, promotes nitrogen retention and increases protein synthesis. This compound is commonly used for overall growth of muscle and to promote growth in body parts that are not up to par with the rest of the user's physique. Results usually depend on dosage. Fat loss and strength increases are not typically seen with MGF's use (as they are in IGF-1 use).
The PEG itself is safe for use as it is approved by the US Food and Drug Administration (FDA) and does not react in the body. The PEG is not broken down in the body and excreted (intact) through urine or feces. Any risk associated PEGylated drugs is due to drug itself not the PEG per se.
Technical Data
In a study on older rodents, muscle fiber reduction in their older muscles was found to be attributed to decreased activity of satellite cells (1). After a certain size was reached, growth ceased. In the presence of MGF, satellite cells became activated and hypertrophy in mature muscles continued.
In experiments where MGF was administered intramuscularly, there was a 20% increase in the weight of the injected muscle fibers within 2 weeks (2). In further studies, it took 4 months for IGF to cause a 25% increase in muscle mass (3). MGF was found to be more potent than IGF-1Ea in rapid muscle growth (4).
[Note: This data is on ***8220;regular***8221; MGF, not the Pegylated version***8230;.we can assume similar results, however]
User Notes
Although the science looks impressive on paper, in the real world, we see something totally different. While PEGMGF should have theoretically given the athletes who use it better results than regular MGF, it struggles to provide even the same results at a higher dosage (judging from the athletes I have personally spoken to).
So does that mean it***8217;s useless?
No, not at all. Not entirely***8230;
I think that the PEGylation is actually a potentially useful addition to MGF if properly used. If we assume that the PEGylation will extend the life of the MGF in the body somewhat, then we can use it in a very specific manner to help our gains. It is nowhere near as good as regular MGF though, and I wouldn***8217;t use it unless I really had the disposable cash on hand.
I feel that, based on conversations with several athletes and bodybuilders, that PEGMGF is best used in conjunction with (not instead of) regular MGF (and IGF). I feel that if one were to use my Peptides protocol (to read about that in detail, check out the article ***8220;Peptides: The Next Frontier in Hypertrophy***8221") , I think that PEGMGF is probably best used on off-days from training, to keep MGF levels elevated and get additional hypertrophy from the longer releasing PEGMGF.
, I think that PEGMGF is probably best used on off-days from training, to keep MGF levels elevated and get additional hypertrophy from the longer releasing PEGMGF.
So, along with regular MGF and Lr3IGF-1, if I felt it to be necessary, I might throw in some PEGMGF on off-days from training, to get additional growth (and again, if it were me, I***8217;d probably recommend 400-500mcg of PEGMGF on off days, with a regular dose of 200mcg of regular MGF + 100mgs of Lr3IGF-1 on training days, as per my article).
For most athletes I***8217;ve spoken to and worked with, this is what we***8217;ve found to be optimal. Again, though***8230;I***8217;m not very fond of this product, and it***8217;s best used (if at all), as a possible adjunct to an IGF + MGF cycle, and never in place of regular MGF. Unfortunately, it just didn***8217;t pan out as people hoped it would, but it***8217;s not a complete waste of money.
References
Chakravarthy et al. 2000
Goldspink, 2001
Musaro et al. 2001
Musaro et al. 2001
MGF is a splice variant of the IGF gene which increases stem cell count in the muscle and allows for muscle fibers to fuse and mature. This is a process required for growth of adult muscle. Natural MGF is made locally and does not travel into the bloodstream. Synthetic MGF is water based and when administered intramuscularly, travels into the bloodstream. MGF is only stable in the blood stream for only a few minutes.
Multiple medical studies have verified the swiftly enhanced muscle growth, rapid recovery from intense training, and incredible fat loss properties of the remarkably fast-acting Pituitary Growth Hormone formula. Order today and start seeing incredible improvement in your general health and overall well-being!
PEGylation is the act of attaching a Polyethylene glycol (PEG) structure to another larger molecule (in this case, MGF). The PEG acts as a protective coating and the theory here is that this will allow the MGF to be carried through the blood stream without being broken down.
Background
I have to be honest here, and say that in my estimation, PEGylating MGF is basically something a research chemical company did to have a bit of a market with no competition for awhile. That***8217;s not to say that it***8217;s not a decent product, but honestly, in this particular case, I feel that marketing was in the drivers seat with the development of this version of MGF, and science was in the backseat asking ***8220;are we there yet?***8221;.
Action
MGF is produced biologically when muscle fibers are broken down through resistance (weight training). It is a potent factor in muscle growth. MGF stimulates muscle growth, creates new muscle fibers, promotes nitrogen retention and increases protein synthesis. This compound is commonly used for overall growth of muscle and to promote growth in body parts that are not up to par with the rest of the user's physique. Results usually depend on dosage. Fat loss and strength increases are not typically seen with MGF's use (as they are in IGF-1 use).
The PEG itself is safe for use as it is approved by the US Food and Drug Administration (FDA) and does not react in the body. The PEG is not broken down in the body and excreted (intact) through urine or feces. Any risk associated PEGylated drugs is due to drug itself not the PEG per se.
Technical Data
In a study on older rodents, muscle fiber reduction in their older muscles was found to be attributed to decreased activity of satellite cells (1). After a certain size was reached, growth ceased. In the presence of MGF, satellite cells became activated and hypertrophy in mature muscles continued.
In experiments where MGF was administered intramuscularly, there was a 20% increase in the weight of the injected muscle fibers within 2 weeks (2). In further studies, it took 4 months for IGF to cause a 25% increase in muscle mass (3). MGF was found to be more potent than IGF-1Ea in rapid muscle growth (4).
[Note: This data is on ***8220;regular***8221; MGF, not the Pegylated version***8230;.we can assume similar results, however]
User Notes
Although the science looks impressive on paper, in the real world, we see something totally different. While PEGMGF should have theoretically given the athletes who use it better results than regular MGF, it struggles to provide even the same results at a higher dosage (judging from the athletes I have personally spoken to).
So does that mean it***8217;s useless?
No, not at all. Not entirely***8230;
I think that the PEGylation is actually a potentially useful addition to MGF if properly used. If we assume that the PEGylation will extend the life of the MGF in the body somewhat, then we can use it in a very specific manner to help our gains. It is nowhere near as good as regular MGF though, and I wouldn***8217;t use it unless I really had the disposable cash on hand.
I feel that, based on conversations with several athletes and bodybuilders, that PEGMGF is best used in conjunction with (not instead of) regular MGF (and IGF). I feel that if one were to use my Peptides protocol (to read about that in detail, check out the article ***8220;Peptides: The Next Frontier in Hypertrophy***8221
, I think that PEGMGF is probably best used on off-days from training, to keep MGF levels elevated and get additional hypertrophy from the longer releasing PEGMGF.So, along with regular MGF and Lr3IGF-1, if I felt it to be necessary, I might throw in some PEGMGF on off-days from training, to get additional growth (and again, if it were me, I***8217;d probably recommend 400-500mcg of PEGMGF on off days, with a regular dose of 200mcg of regular MGF + 100mgs of Lr3IGF-1 on training days, as per my article).
For most athletes I***8217;ve spoken to and worked with, this is what we***8217;ve found to be optimal. Again, though***8230;I***8217;m not very fond of this product, and it***8217;s best used (if at all), as a possible adjunct to an IGF + MGF cycle, and never in place of regular MGF. Unfortunately, it just didn***8217;t pan out as people hoped it would, but it***8217;s not a complete waste of money.
References
Chakravarthy et al. 2000
Goldspink, 2001
Musaro et al. 2001
Musaro et al. 2001
vibrant
CHEMICALLY ENGINEERED
Short article (I dont know who the author is)
The Truth about Peptides
The TRUTH about peptides and HOW they will help YOU achieve your long term goal
The truth about peptides (what to expect)
For all who have been misinformed or mislead about these cutting edge supplements, or those just getting interested, this is a must read
For all the people out there that looking for instant gratification, these may not be your supplement of choice. But for the guys that are willing to go and bust our butts in the gym day in and day out and we don't need to see an inch added our arms this week to come back and do it again next week because we know that if you keep coming back that***8217;s where the true rewards begin.
Don't be fooled by other companies advertising steroid like effects from peptides like mgf or IGF or any type of GH. It***8217;s a false claim made to make sales. And its place/people like this that are ruining the peptide business. People don't see anything close to the results they got from their last cycle of AAS and immediately think they got screwed or scammed or that peptides are junk and a waste of money. This is the fault of the seller for not informing the client.
When you do a cycle of AAS, what***8217;s next?? pct of course. All AAS users have the same fears at the end of each cycle. They don't want to lose their hard earned gains. The gains that came so fast and so easy, but can be lost in the blink of an eye without proper post cycle therapy (pct). And even with good pct it***8217;s still hard to keep everything. Then there is the other evil. estrogen!!! You are popping anti-e's and AI's and progestin blockers that cost you a ton extra because you don***8217;t want those ***** tits or that bloat, or the sudden fat gain. AAS = great gains, followed by anxiety. Now I'm not going to knock AAS they are a cornerstone. They give undeniable results. But at the cost of side effects, and pct anxiety and cost. So they aren***8217;t perfect. You spend your off time trying to maintain, let alone trying to make gains....
Now let***8217;s look at what happens during a cycle of peptides. Taken right with good diet and exercise just like you would for an AAS, but maybe not quite as many calories as some do on heavy cycles, you will see some small gains, some leaning out, but no where near the 20lbs of beef you put on last test/tren cycle. You might be lucky with 5lbs over the course of 6-8 weeks. But here is where it gets good. All those gains, there yours, not going anywhere, not going to suddenly start to subside, they aren***8217;t going to result in some post cycle bloat, ***** tit formation, or fat gain. In fact your metabolism will be slightly higher from the gains. Anxiety free... no wait!!! It***8217;s better than anxiety free; you should be just as stoked now as when you started the cycle. Because after you do a cycle of peptides like IGF or mgf especially. The gains are going to come better after the cycle then they did before. Unlike AAS where you try to gain and then maintain.
You see steroids make the adult muscle cells (myotubules) bigger, but the bigger these cells get as we all know the harder and harder it is to make them even bigger. These myotubules are limited in size by the amount of nuclei they contain. The closer they get to being maxed the harder for them to grow and when they are maxed well that***8217;s about it.... gains will be few and far between. Myotubules don't divide like other cells so you pretty much have as many as you***8217;re going to have for the most part. Hyperplasia does occur but it is a very rare process. This is where some people refer to the genetics. Because your genetics determines largely your # of myotubules you have, and the hormones that regulate them.
This is where peptides make their mark. Growth factors in short lead to an increase in the potential of the myotubules to grow because they can influence the stem cell pools of the muscle which are their for growth and repair, to fuse with the adult myotubules and increase the # of nuclei. This means they can grow more again, and grow easier. Individual mechanisms for each peptide may very, but this is the overall effect they are all going for. So after taking some peptides you will experience better gains than before, with relatively non existent side effects, no PTC, no anxiety. These are supplements with an investment in mind, a future goal beyond the current cycle, and realistic view that real gains don't have to come in 6-12 week segments but can come all year round.
When you add all that up, the cost of peptides is not as far overhead as you might think. It cost a lot of money to bring this caliber of products to the market. Peptides are complicated structures, not simple molecules like AAS. But if you in this business for the long hall, peptides have extremely good benefits to offer.
The Truth about Peptides
The TRUTH about peptides and HOW they will help YOU achieve your long term goal
The truth about peptides (what to expect)
For all who have been misinformed or mislead about these cutting edge supplements, or those just getting interested, this is a must read
For all the people out there that looking for instant gratification, these may not be your supplement of choice. But for the guys that are willing to go and bust our butts in the gym day in and day out and we don't need to see an inch added our arms this week to come back and do it again next week because we know that if you keep coming back that***8217;s where the true rewards begin.
Don't be fooled by other companies advertising steroid like effects from peptides like mgf or IGF or any type of GH. It***8217;s a false claim made to make sales. And its place/people like this that are ruining the peptide business. People don't see anything close to the results they got from their last cycle of AAS and immediately think they got screwed or scammed or that peptides are junk and a waste of money. This is the fault of the seller for not informing the client.
When you do a cycle of AAS, what***8217;s next?? pct of course. All AAS users have the same fears at the end of each cycle. They don't want to lose their hard earned gains. The gains that came so fast and so easy, but can be lost in the blink of an eye without proper post cycle therapy (pct). And even with good pct it***8217;s still hard to keep everything. Then there is the other evil. estrogen!!! You are popping anti-e's and AI's and progestin blockers that cost you a ton extra because you don***8217;t want those ***** tits or that bloat, or the sudden fat gain. AAS = great gains, followed by anxiety. Now I'm not going to knock AAS they are a cornerstone. They give undeniable results. But at the cost of side effects, and pct anxiety and cost. So they aren***8217;t perfect. You spend your off time trying to maintain, let alone trying to make gains....
Now let***8217;s look at what happens during a cycle of peptides. Taken right with good diet and exercise just like you would for an AAS, but maybe not quite as many calories as some do on heavy cycles, you will see some small gains, some leaning out, but no where near the 20lbs of beef you put on last test/tren cycle. You might be lucky with 5lbs over the course of 6-8 weeks. But here is where it gets good. All those gains, there yours, not going anywhere, not going to suddenly start to subside, they aren***8217;t going to result in some post cycle bloat, ***** tit formation, or fat gain. In fact your metabolism will be slightly higher from the gains. Anxiety free... no wait!!! It***8217;s better than anxiety free; you should be just as stoked now as when you started the cycle. Because after you do a cycle of peptides like IGF or mgf especially. The gains are going to come better after the cycle then they did before. Unlike AAS where you try to gain and then maintain.
You see steroids make the adult muscle cells (myotubules) bigger, but the bigger these cells get as we all know the harder and harder it is to make them even bigger. These myotubules are limited in size by the amount of nuclei they contain. The closer they get to being maxed the harder for them to grow and when they are maxed well that***8217;s about it.... gains will be few and far between. Myotubules don't divide like other cells so you pretty much have as many as you***8217;re going to have for the most part. Hyperplasia does occur but it is a very rare process. This is where some people refer to the genetics. Because your genetics determines largely your # of myotubules you have, and the hormones that regulate them.
This is where peptides make their mark. Growth factors in short lead to an increase in the potential of the myotubules to grow because they can influence the stem cell pools of the muscle which are their for growth and repair, to fuse with the adult myotubules and increase the # of nuclei. This means they can grow more again, and grow easier. Individual mechanisms for each peptide may very, but this is the overall effect they are all going for. So after taking some peptides you will experience better gains than before, with relatively non existent side effects, no PTC, no anxiety. These are supplements with an investment in mind, a future goal beyond the current cycle, and realistic view that real gains don't have to come in 6-12 week segments but can come all year round.
When you add all that up, the cost of peptides is not as far overhead as you might think. It cost a lot of money to bring this caliber of products to the market. Peptides are complicated structures, not simple molecules like AAS. But if you in this business for the long hall, peptides have extremely good benefits to offer.
vibrant
CHEMICALLY ENGINEERED
Written by DatBtrue
"Introduction to Natural GH Release and GHRH +GHRP...
Introduction to natural GH release and GHRH/GHRPs
Introduction to the thread
What is growth hormone?
Synthetic Growth Hormone is an artificially created hormone "identical" to the major naturally produced (endogenous) isoform. It is often referred to by its molecular mass which is 22kDa (kilodaltons) and is made up of a sequence of 191 amino acids (primary structure) with a very specific folding pattern that comprise a three-dimensional structure (tertiary structure). This tertiary structure is subject to potential shape change through a process known as thermal denaturation. While many labs are capable of generating growth hormone (GH) with the proper primary structure not all will be capable of creating a tertiary structure identical to the major naturally occurring growth hormone. The tertiary structure can determine the strength with which the growth hormone molecule binds to a receptor which will in turn affect the "strength" of the intracellular signaling which mediates the events leading to protein transcription, metabolism, IGF-1 creation, etc. It is this inconsistency that accounts in part for the differences in effectiveness of various non-pharmaceutically produced synthetic growth hormone.
Naturally produced Growth Hormone is produced in the anterior pituitary and to a far lesser extent in peripheral tissue. It is made up of a blend of isoforms the majority of which is the 22kDa (191 amino acid) variety with which most are familiar. In addition an isoform that is missing the 15 amino acids that interact with the prolactin receptor is also produced. This form is known as 20kDa and although it binds differently to the growth hormone receptor it has been shown to be equally potent to 22kDa. It appears that 20kDa has lower diabetogenic activity then 22kDa. The pituitary releases a blend of these two isoforms with 20kDa averaging perhaps 10% of the total although this percentage increases post-exercise. Currently there is no synthetic produced for external administration for this isoform.
Growth hormone (GH) in the body is released in pulsatile fashion. It has been demonstrated that this pattern promotes growth. The pituitary is capable of rather quickly synthesizing very large amounts of growth hormone which it stores large amounts in both a finished and unfinished form. Adults rarely experience GH pulses (i.e. releases of pituitary stores) that completely deplete these stores. As we age we do not lose the ability to create and store large amounts of growth hormone. Rather we experience a diminished capacity to "instruct" their release. The volume of GH that is released can not be properly equated to the exogenous administration of synthetic GH for the reason that a set of behavioral characteristics accompany natural GH that differ from those of synthetic GH. Among those characteristics are concentrated pulsatile release which upon binding in mass to growth hormone receptors on the surface of cells initiate signaling cascades which mediate growth events by translocating signaling proteins to the nucleus of the cell where protein transcription and metabolic events occur.
These very important signaling pathways desensitize to Growth Hormone's initiating effects and need to experience an absence of Growth Hormone in order to reset and be ready to act again. The presence of GH released in pulsatile fashion is graphed as a wave with the low or no growth hormone period graphed as a trough. Therefore attempting to find a natural GH to synthetic GH equivalency is not very productive because in the end what is probably import is:
- the quantity & quality of intracellular signaling events; and
- the degree to which GH stimulates autocrine/paracrine (locally produced/locally used) muscle IGF-1 & post-exercise its splice variant MGF.
Brief overview of natural GH release
The initiation of growth hormone release in the pituitary is dependent on a trilogy of hormones:
Somatostatin which is the inhibitory hormone and responsible in large part for the creation of pulsation;
Growth Hormone Releasing Hormone (GHRH) which is the stimulatory hormone responsible for initiating GH release; and
Ghrelin which is a modulating hormone and in essence optimizes the balance between the "on" hormone & the "off" hormone. Before Ghrelin was discovered the synthetic growth hormone releasing peptides (GHRPs) were created and are superior to Ghrelin in that they do not share Ghrelin's lipogenic behavior. These GHRPs are GHRP-6, GHRP-2, Hexarelin and later Ipamorelin all of which behave in similar fashion.
In the aging adult these Ghrelin-mimetics or the GHRPs restore a more youthful ability to release GH from the pituitary as they turn down somatostatin's negative influence which becomes stronger as we age and turn up growth hormone releasing hormone's influence which becomes weaker as we age.
The exogenous administration of Growth Hormone Releasing Hormone (GHRH) creates a pulse of GH release which will be small if administered during a natural GH trough and higher if administered during a rising natural GH wave.
Growth Hormone Releasing Peptides (GHRP-6, GHRP-2, Ipamorelin) are capable of creating a larger pulse of GH on their own then GHRH and they do this with much more consistency and predictability without regard to whether a natural wave or trough of GH is currently taking place.
Synergy of GHRH + GHRP
It is well documented and established that the concurrent administration of Growth Hormone Releasing Hormone (GHRH) and a Growth Hormone Releasing Peptide (GHRP-6, GHRP-2 or Ipamorelin) results in synergistic release of GH from pituitary stores. In other words if GHRH contributes a GH amount quantified as the number 2 and GHRPs contributed a GH amount quantified as the number 4 the total GH release is not additive (i.e. 2 + 4 = 6). Rather the whole is greater than the sum of the parts such that 2 + 4 = 10.
While the GHRPs (GHRP-6, GHRP-2 and Ipamorelin) come in only one half-life form and are capable of generating a GH pulse that lasts a couple of hours re-administration of a GHRPis required to effect additional pulses.
Growth Hormone Releasing Hormone (GHRH) however is currently available in several forms which vary only by their half-lives. Naturally occurring GHRH is either a 40 or 44 amino acid peptide with the bioactive portion residing in the first 29 amino acids. This shortened peptide identical in behavior and half-life to that of GHRH is called Growth Hormone Releasing Factor and is abbreviated as GRF(1-29).
GRF(1-29) is produced and sold as a drug called Sermorelin. It has a short-half life measured in minutes. If you prefer analogies think of this as a Testosterone Suspension (i.e. unestered).
To increase the stability and half-life of GRF(1-29) four amino acid changes where made to its structure. These changes increase the half-life beyond 30 minutes which is more than sufficient to exert a sustained effect which will maximize a GH pulse. This form is often called tetrasubstituted GRF(1-29) (or modified) and unfortunately & confusingly mislabeled as CJC-1295. If you prefer analogies think of this as a Testosterone Propionate (i.e. short-estered).
Note that some may also refer to this as CJC-1295 without the DAC (Drug Affinity Complex).
Frequent dosing of either the aforementioned modified GRF(1-29) or regular GRF(1-29) is required and as previously indicated works synergistically with a GHRP.
In an attempt to create a more convenient long-lasting GHRH, a compound known as CJC-1295 was created. This compound is identical to the aforementioned modified GRF(1-29) with the addition of the amino acid Lysine which links to a non-peptide molecule known as a "Drug Affinity Complex (DAC)". This complex allows GRF(1-29) to bind to albumin post-injection in plasma and extends its half-life to that of days. If you prefer analogies think of this as a Testosterone Cypionate (i.e. long-estered). Unfortunately CJC-1295 results in growth hormone bleed. This means that although pulsation remains base levels end up chronically elevated.
You do not want to use CJC-1295. You want to use Modified GRF(1-29).
Why? (Partial Explanation)
"Cell-to-cell communication is also likely to reflect the density and proximity of adjacent cells as GH responsiveness (but not sensitivity) to GHRH is enhanced at higher densities and basal GH release is greatest at low densities."
"Cell-to-cell contact may therefore affect the cellular integrity of somatotrophs because GH synthesis or secretory granule storage may be better maintained in high density cell concentration then in low-density concentrations." - Growth Hormone, Stephen Harvey
What happens is cells in the pituitary communicate. They self organize and create a firing network for coordinated growth hormone release. This communication creates a high density of GH releasing cells. They are in close proximity through their communicatory network. The cells have specific spatial relationships that may be modulated by peripheral endocrines. These include sex steroids, thyroid hormones, glucorticoids and even the pancreatic and gut hormones. Their spatial relationship is also effected by physiological state such as nutrient status, age and pregnancy.
As a quick example, corticotroph, thyrotrophs and folliculostellate cells are in close proximity to somatotrophs and communicate with them through gap junctions (almost like just reaching out and touching signaling). They have the potential to effect and be effected by their neighbors.
What happens when you have GHRH always around is you force these somatotrophs to release GH because they are sensitive to the GHRH binding to them and effecting release. By constantly occupying you are preventing them from coordinating with surrounding cell populations. You force these cells to act as low density subpopulations. Basal GH release is greatest when you can disperse the spatial relationship between somatotrophs and that is what an always on GHRH will do.
CJC-1295 as an always on GHRH will force upon somatotrophs loner behavior with a single constant chore. This reduces GH responsiveness as this only occurs when somatotrophs can communicate, self organize and maintain social relationships with the surrounding community. These types of social somatotrophs are better able to make and store GH then the loner cells.
So CJC-1295 seems to disperse somatotrophs and enslave them getting less from them then if it had just let them congregate in towns and cities.
Aging has an effect on the vitality of city centers as well and as we age these somatotroph population centers become less vigorous. By using a more physiological GHRH such as modified GRF(1-29) together with a modulator GHRP-2 we revitalize that inner city and allow our cells to be more social and thus more productive. If instead we choose to use CJC-1295 we not only fail to remedy the problem associated with age , but we may end up exacerbating it.
I conjecture that it also makes them better neighbors to corticotroph, thyrotrophs and folliculostellate cells as well.
What follows is:
A Basic Peptide Primer (which introduces the concept & structure of peptides)
A Brief Summary of Dosing and Administration (for someone that wants to know the "how to use" straight away)
If all of this is a bit unclear because a lot of new concepts are thrown at you the following original article should help:
Growth Hormone Secretagogues
I have only one pet-peeve and that is when someone refers to synthetic growth hormone as "real" growth hormone. The GH that your body produces is as real as it gets. It is what grew you from a fetus to a boy (girl) and from a boy (girl) to a man (woman). - DatBtrue
"Introduction to Natural GH Release and GHRH +GHRP...
Introduction to natural GH release and GHRH/GHRPs
Introduction to the thread
What is growth hormone?
Synthetic Growth Hormone is an artificially created hormone "identical" to the major naturally produced (endogenous) isoform. It is often referred to by its molecular mass which is 22kDa (kilodaltons) and is made up of a sequence of 191 amino acids (primary structure) with a very specific folding pattern that comprise a three-dimensional structure (tertiary structure). This tertiary structure is subject to potential shape change through a process known as thermal denaturation. While many labs are capable of generating growth hormone (GH) with the proper primary structure not all will be capable of creating a tertiary structure identical to the major naturally occurring growth hormone. The tertiary structure can determine the strength with which the growth hormone molecule binds to a receptor which will in turn affect the "strength" of the intracellular signaling which mediates the events leading to protein transcription, metabolism, IGF-1 creation, etc. It is this inconsistency that accounts in part for the differences in effectiveness of various non-pharmaceutically produced synthetic growth hormone.
Naturally produced Growth Hormone is produced in the anterior pituitary and to a far lesser extent in peripheral tissue. It is made up of a blend of isoforms the majority of which is the 22kDa (191 amino acid) variety with which most are familiar. In addition an isoform that is missing the 15 amino acids that interact with the prolactin receptor is also produced. This form is known as 20kDa and although it binds differently to the growth hormone receptor it has been shown to be equally potent to 22kDa. It appears that 20kDa has lower diabetogenic activity then 22kDa. The pituitary releases a blend of these two isoforms with 20kDa averaging perhaps 10% of the total although this percentage increases post-exercise. Currently there is no synthetic produced for external administration for this isoform.
Growth hormone (GH) in the body is released in pulsatile fashion. It has been demonstrated that this pattern promotes growth. The pituitary is capable of rather quickly synthesizing very large amounts of growth hormone which it stores large amounts in both a finished and unfinished form. Adults rarely experience GH pulses (i.e. releases of pituitary stores) that completely deplete these stores. As we age we do not lose the ability to create and store large amounts of growth hormone. Rather we experience a diminished capacity to "instruct" their release. The volume of GH that is released can not be properly equated to the exogenous administration of synthetic GH for the reason that a set of behavioral characteristics accompany natural GH that differ from those of synthetic GH. Among those characteristics are concentrated pulsatile release which upon binding in mass to growth hormone receptors on the surface of cells initiate signaling cascades which mediate growth events by translocating signaling proteins to the nucleus of the cell where protein transcription and metabolic events occur.
These very important signaling pathways desensitize to Growth Hormone's initiating effects and need to experience an absence of Growth Hormone in order to reset and be ready to act again. The presence of GH released in pulsatile fashion is graphed as a wave with the low or no growth hormone period graphed as a trough. Therefore attempting to find a natural GH to synthetic GH equivalency is not very productive because in the end what is probably import is:
- the quantity & quality of intracellular signaling events; and
- the degree to which GH stimulates autocrine/paracrine (locally produced/locally used) muscle IGF-1 & post-exercise its splice variant MGF.
Brief overview of natural GH release
The initiation of growth hormone release in the pituitary is dependent on a trilogy of hormones:
Somatostatin which is the inhibitory hormone and responsible in large part for the creation of pulsation;
Growth Hormone Releasing Hormone (GHRH) which is the stimulatory hormone responsible for initiating GH release; and
Ghrelin which is a modulating hormone and in essence optimizes the balance between the "on" hormone & the "off" hormone. Before Ghrelin was discovered the synthetic growth hormone releasing peptides (GHRPs) were created and are superior to Ghrelin in that they do not share Ghrelin's lipogenic behavior. These GHRPs are GHRP-6, GHRP-2, Hexarelin and later Ipamorelin all of which behave in similar fashion.
In the aging adult these Ghrelin-mimetics or the GHRPs restore a more youthful ability to release GH from the pituitary as they turn down somatostatin's negative influence which becomes stronger as we age and turn up growth hormone releasing hormone's influence which becomes weaker as we age.
The exogenous administration of Growth Hormone Releasing Hormone (GHRH) creates a pulse of GH release which will be small if administered during a natural GH trough and higher if administered during a rising natural GH wave.
Growth Hormone Releasing Peptides (GHRP-6, GHRP-2, Ipamorelin) are capable of creating a larger pulse of GH on their own then GHRH and they do this with much more consistency and predictability without regard to whether a natural wave or trough of GH is currently taking place.
Synergy of GHRH + GHRP
It is well documented and established that the concurrent administration of Growth Hormone Releasing Hormone (GHRH) and a Growth Hormone Releasing Peptide (GHRP-6, GHRP-2 or Ipamorelin) results in synergistic release of GH from pituitary stores. In other words if GHRH contributes a GH amount quantified as the number 2 and GHRPs contributed a GH amount quantified as the number 4 the total GH release is not additive (i.e. 2 + 4 = 6). Rather the whole is greater than the sum of the parts such that 2 + 4 = 10.
While the GHRPs (GHRP-6, GHRP-2 and Ipamorelin) come in only one half-life form and are capable of generating a GH pulse that lasts a couple of hours re-administration of a GHRPis required to effect additional pulses.
Growth Hormone Releasing Hormone (GHRH) however is currently available in several forms which vary only by their half-lives. Naturally occurring GHRH is either a 40 or 44 amino acid peptide with the bioactive portion residing in the first 29 amino acids. This shortened peptide identical in behavior and half-life to that of GHRH is called Growth Hormone Releasing Factor and is abbreviated as GRF(1-29).
GRF(1-29) is produced and sold as a drug called Sermorelin. It has a short-half life measured in minutes. If you prefer analogies think of this as a Testosterone Suspension (i.e. unestered).
To increase the stability and half-life of GRF(1-29) four amino acid changes where made to its structure. These changes increase the half-life beyond 30 minutes which is more than sufficient to exert a sustained effect which will maximize a GH pulse. This form is often called tetrasubstituted GRF(1-29) (or modified) and unfortunately & confusingly mislabeled as CJC-1295. If you prefer analogies think of this as a Testosterone Propionate (i.e. short-estered).
Note that some may also refer to this as CJC-1295 without the DAC (Drug Affinity Complex).
Frequent dosing of either the aforementioned modified GRF(1-29) or regular GRF(1-29) is required and as previously indicated works synergistically with a GHRP.
In an attempt to create a more convenient long-lasting GHRH, a compound known as CJC-1295 was created. This compound is identical to the aforementioned modified GRF(1-29) with the addition of the amino acid Lysine which links to a non-peptide molecule known as a "Drug Affinity Complex (DAC)". This complex allows GRF(1-29) to bind to albumin post-injection in plasma and extends its half-life to that of days. If you prefer analogies think of this as a Testosterone Cypionate (i.e. long-estered). Unfortunately CJC-1295 results in growth hormone bleed. This means that although pulsation remains base levels end up chronically elevated.
You do not want to use CJC-1295. You want to use Modified GRF(1-29).
Why? (Partial Explanation)
"Cell-to-cell communication is also likely to reflect the density and proximity of adjacent cells as GH responsiveness (but not sensitivity) to GHRH is enhanced at higher densities and basal GH release is greatest at low densities."
"Cell-to-cell contact may therefore affect the cellular integrity of somatotrophs because GH synthesis or secretory granule storage may be better maintained in high density cell concentration then in low-density concentrations." - Growth Hormone, Stephen Harvey
What happens is cells in the pituitary communicate. They self organize and create a firing network for coordinated growth hormone release. This communication creates a high density of GH releasing cells. They are in close proximity through their communicatory network. The cells have specific spatial relationships that may be modulated by peripheral endocrines. These include sex steroids, thyroid hormones, glucorticoids and even the pancreatic and gut hormones. Their spatial relationship is also effected by physiological state such as nutrient status, age and pregnancy.
As a quick example, corticotroph, thyrotrophs and folliculostellate cells are in close proximity to somatotrophs and communicate with them through gap junctions (almost like just reaching out and touching signaling). They have the potential to effect and be effected by their neighbors.
What happens when you have GHRH always around is you force these somatotrophs to release GH because they are sensitive to the GHRH binding to them and effecting release. By constantly occupying you are preventing them from coordinating with surrounding cell populations. You force these cells to act as low density subpopulations. Basal GH release is greatest when you can disperse the spatial relationship between somatotrophs and that is what an always on GHRH will do.
CJC-1295 as an always on GHRH will force upon somatotrophs loner behavior with a single constant chore. This reduces GH responsiveness as this only occurs when somatotrophs can communicate, self organize and maintain social relationships with the surrounding community. These types of social somatotrophs are better able to make and store GH then the loner cells.
So CJC-1295 seems to disperse somatotrophs and enslave them getting less from them then if it had just let them congregate in towns and cities.
Aging has an effect on the vitality of city centers as well and as we age these somatotroph population centers become less vigorous. By using a more physiological GHRH such as modified GRF(1-29) together with a modulator GHRP-2 we revitalize that inner city and allow our cells to be more social and thus more productive. If instead we choose to use CJC-1295 we not only fail to remedy the problem associated with age , but we may end up exacerbating it.
I conjecture that it also makes them better neighbors to corticotroph, thyrotrophs and folliculostellate cells as well.
What follows is:
A Basic Peptide Primer (which introduces the concept & structure of peptides)
A Brief Summary of Dosing and Administration (for someone that wants to know the "how to use" straight away)
If all of this is a bit unclear because a lot of new concepts are thrown at you the following original article should help:
Growth Hormone Secretagogues
I have only one pet-peeve and that is when someone refers to synthetic growth hormone as "real" growth hormone. The GH that your body produces is as real as it gets. It is what grew you from a fetus to a boy (girl) and from a boy (girl) to a man (woman). - DatBtrue
Phatbastard
Knowledge Equals Results
Great Compilation of Info Vibrant
Ezskanken
New member
Another post borrowed from Dat regarding what to take/not take after administration to prevent blunting GH release...
Protein does not blunt GHRH activity (i.e. Mod GRF(1-29))
Protein does not blunt GHRP activity (i.e. GHRP-6, GHRP-2, Ipamorelin)
Carbs strongly blunt GHRH activity (i.e. Mod GRF(1-29))
Carbs only partially blunt GHRP activity (i.e. GHRP-6, GHRP-2, Ipamorelin)
Fats strongly blunt GHRH activity (i.e. Mod GRF(1-29))
Fats strongly blunt GHRP activity (i.e. GHRP-6, GHRP-2, Ipamorelin)
T-0 -----------------------T-10------------------------T-20-------------------------T-30
<<<<<<<<<Protein>>>>>>>>><<<<<<<<<<<<<<<Carbs>>>>> >>>>>>>>><<<<<<Fats>>>>>>
Protein does not blunt GHRH activity (i.e. Mod GRF(1-29))
Protein does not blunt GHRP activity (i.e. GHRP-6, GHRP-2, Ipamorelin)
Carbs strongly blunt GHRH activity (i.e. Mod GRF(1-29))
Carbs only partially blunt GHRP activity (i.e. GHRP-6, GHRP-2, Ipamorelin)
Fats strongly blunt GHRH activity (i.e. Mod GRF(1-29))
Fats strongly blunt GHRP activity (i.e. GHRP-6, GHRP-2, Ipamorelin)
T-0 -----------------------T-10------------------------T-20-------------------------T-30
<<<<<<<<<Protein>>>>>>>>><<<<<<<<<<<<<<<Carbs>>>>> >>>>>>>>><<<<<<Fats>>>>>>
Ezskanken
New member
Another post borrowed from Dat I think will be extremely useful...
A Brief Summary of Dosing and Administration
Dosing GHRPs
The saturation dose in most studies on the GHRPs (GHRP-6, GHRP-2, Ipamorelin & Hexarelin) is defined as either 100mcg or 1mcg/kg.
What that means is that 100mcg will saturate the receptors fully, but if you add another 100mcg to that dose only 50% of that portion will be effective. If you add an additional 100mcg to that dose only about 25% will be effective. Perhaps a final 100mcg might add a little something to GH release but that is it.
So 100mcg is the saturation dose and you could add more up to 300 to 400mcg and get a little more effect.
A 500mcg dose will not be more effective then a 400mcg, perhaps not even more effective then 300mcg.
The additional problems are desensitization & cortisol/prolactin side-effects.
Ipamorelin is about as efficacious as GHRP-6 in causing GH release but even at higher dose (above 100mcg) it does not create prolactin or cortisol.
GHRP-6 at the saturation dose 100mcg does not really increase prolactin & cortisol but may do so slightly at higher doses. This rise is still within the normal range.
GHRP-2 is more efficacious then GHRP-6 at causing GH release but at the saturation dose or higher may produce a slight to moderate increase in prolactin & cortisol. This rise is still within the normal range although doses of 200 - 400mcg might make it the high end of the normal range.
Hexarelin in some is the most efficacious otherwise it is equipotent or a little less so then GHRP-2 at causing an increase in GH release. However it has the highest potential to also increase cortisol & prolactin. This rise will occur even at the 100mcg saturation dose. This rise will reach the higher levels of what is defined as normal.
Desensitization
GHRP-6 can be used at saturation dose (100mcg) three or four times a day without risk of desensitization.
GHRP-2 at saturation dose several times a day will not result in desensitization.
Hexarelin has been shown to bring about desensitization but in a long-term study the pituitary recovered its sensitivity so that there was not long-term loss of sensitivity at saturation dose. However dosing Hexarelin even at 100mcg three times a day will likely lead to some down regulation within 14 days.
If desensitization were to ever occur for any of these GHRPs simply stopping use for several days will remedy this effect.
Chronic use of GHRP-2 at 100mcg dosed several times a day every day will not cause pituitary problems, nor significant prolactin or cortisol problems, nor desensitize.
GHRH
Now Sermorelin, GHRH (1-44) and GRF(1-29) all are basically GHRH and have a short half-life in plasma because of quick cleavage between the 2nd & 3rd amino acid. This is no worry naturally because this hormone is secreted from the hypothalamus and travels a short distance to the underlying anterior pituitary and is not really subject to enzymatic cleavage. The release from the hypothalamus and binding to somatotrophs (pituitary cells) happens quickly.
However when injected into the body it must circulate before finding its way to the pituitary and so within 3 minutes it is already being degraded.
That is why GHRH in the above forms must be dosed high to get an effect.
GHRH analogs
All GHRH analogs swap Alanine at the 2nd position for D-Alanine which makes the peptide resistant to quick cleavage at that position. This means analogs will be more effective when injected at smaller dosing.
The analog tetra or 4 substituted GRF(1-29) sometimes called CJC w/o the DAC or referred to by me as modified GRF(1-29) has other amino acid modifications. They are a glutamine (Gln or Q) at the 8-position, alanine (Ala or A) at the 15-position, and a leucine (Leu or L) at the 27-position.
The alanine at the 8th position enhances bioavailability but the other two amino substitutions are made to enhance the manufacturing process (i.e. create manufacturing stability).
For use in vivo, in humans, the GHRH analog known as CJC w/o the DAC or tetra (4) substituted GRF(1-29) or modified GRF(1-29) is a very effective peptide with a half-life probably 30+ minutes.
That is long enough to be completely effective.
The saturation dose is also defined as 100mcg.
Problem w/ Using any GHRH alone
The problem with using a GHRH even the stronger analogs is that they are only highly effective when somatostatin is low (the GH inhibiting hormone). So if you unluckily administer in a trough (or when a GH pulse is not naturally occurring) you will add very little GH release. If however you luckily administer during a rising wave or GH pulse (somatostatin will not be active at this point) you will add to GH release.
Solution is GHRP + GHRH analog
The solution is simple and highly effective. You administer a GHRH analog with a GHRP. The GHRP creates a pulse of GH. It does this through several mechanisms. One mechanism is the reduction of somatostatin release from the hypothalamus, another is a reduction of somatostatin influence at the pituitary, still another is increased release of GHRH from the brain and finally GHRPs act on the same pituitary cells (somatotrophs) as do GHRHs but use a different mechanism to increase cAMP formation which will further cause GH release from somatotroph stores.
GHRH also has a way of reciprocally reinforcing GHRPs action.
The result is a synergistic GH release.
The GH is not additive it is synergistic. By that I mean:
If GHRH by itself will cause a GH release valued at 2
and GHRP itself will cause a GH release valued at 5
Together the GH is not 7 (5+2) it turns out to say 16!
A solid protocol
A solid protocol would be to use a GHRP + a GHRH analog pre-bed (to support the nightime pulse) and once or twice throughout the day.
For anti-aging, deep restful restorative sleep, the once at night dosing is all you need. For an adult aged 40+ it is enough to restore GH to youthful levels.
However for bodybuilding or fatloss or injury repair multiple dosings can be effective.
The GHRH analog can be used at 100mcg and as high as you want without problems.
The GHRP-2 can always be used at 100mcg w/o problems but a dose of 200mcg will probably be fine as well.
Again desensitization is something to keep an eye on particularly with the highest doses of GHRP-2 and all doses of Hexarelin.
So 100 - 200mcg of GHRP-2 + 100 - 500mcg+ of a GHRH analog taken together will be effective.
This may be dosed several times a day to be highly effective.
A solid approach is a bit more conservative at 100mcg of GHRP-2 + 100mcg of a GHRH analog dosed either once, twice, three or four times a day.
When dosing multiple times a day at least 3 hours should separate the administrations.
The difference is once a day dosing pre-bed will give a youthful restorative amount of GH while multiple dosing and or higher levels will give higher GH & IGF-1 levels when coupled with diet & exercise will lead to muscle gain & fatloss.
Dose w/o food
Administration should ideally be done on either an empty stomach or with only protein in the stomach. Fats & carbs blunt GH release. So administer the peptides and wait about 20 minutes (no more then 30 but no less then 15 minutes) to eat. AT that point the GH pulse has about hit the peak and you can eat what you want.
A Brief Summary of Dosing and Administration
Dosing GHRPs
The saturation dose in most studies on the GHRPs (GHRP-6, GHRP-2, Ipamorelin & Hexarelin) is defined as either 100mcg or 1mcg/kg.
What that means is that 100mcg will saturate the receptors fully, but if you add another 100mcg to that dose only 50% of that portion will be effective. If you add an additional 100mcg to that dose only about 25% will be effective. Perhaps a final 100mcg might add a little something to GH release but that is it.
So 100mcg is the saturation dose and you could add more up to 300 to 400mcg and get a little more effect.
A 500mcg dose will not be more effective then a 400mcg, perhaps not even more effective then 300mcg.
The additional problems are desensitization & cortisol/prolactin side-effects.
Ipamorelin is about as efficacious as GHRP-6 in causing GH release but even at higher dose (above 100mcg) it does not create prolactin or cortisol.
GHRP-6 at the saturation dose 100mcg does not really increase prolactin & cortisol but may do so slightly at higher doses. This rise is still within the normal range.
GHRP-2 is more efficacious then GHRP-6 at causing GH release but at the saturation dose or higher may produce a slight to moderate increase in prolactin & cortisol. This rise is still within the normal range although doses of 200 - 400mcg might make it the high end of the normal range.
Hexarelin in some is the most efficacious otherwise it is equipotent or a little less so then GHRP-2 at causing an increase in GH release. However it has the highest potential to also increase cortisol & prolactin. This rise will occur even at the 100mcg saturation dose. This rise will reach the higher levels of what is defined as normal.
Desensitization
GHRP-6 can be used at saturation dose (100mcg) three or four times a day without risk of desensitization.
GHRP-2 at saturation dose several times a day will not result in desensitization.
Hexarelin has been shown to bring about desensitization but in a long-term study the pituitary recovered its sensitivity so that there was not long-term loss of sensitivity at saturation dose. However dosing Hexarelin even at 100mcg three times a day will likely lead to some down regulation within 14 days.
If desensitization were to ever occur for any of these GHRPs simply stopping use for several days will remedy this effect.
Chronic use of GHRP-2 at 100mcg dosed several times a day every day will not cause pituitary problems, nor significant prolactin or cortisol problems, nor desensitize.
GHRH
Now Sermorelin, GHRH (1-44) and GRF(1-29) all are basically GHRH and have a short half-life in plasma because of quick cleavage between the 2nd & 3rd amino acid. This is no worry naturally because this hormone is secreted from the hypothalamus and travels a short distance to the underlying anterior pituitary and is not really subject to enzymatic cleavage. The release from the hypothalamus and binding to somatotrophs (pituitary cells) happens quickly.
However when injected into the body it must circulate before finding its way to the pituitary and so within 3 minutes it is already being degraded.
That is why GHRH in the above forms must be dosed high to get an effect.
GHRH analogs
All GHRH analogs swap Alanine at the 2nd position for D-Alanine which makes the peptide resistant to quick cleavage at that position. This means analogs will be more effective when injected at smaller dosing.
The analog tetra or 4 substituted GRF(1-29) sometimes called CJC w/o the DAC or referred to by me as modified GRF(1-29) has other amino acid modifications. They are a glutamine (Gln or Q) at the 8-position, alanine (Ala or A) at the 15-position, and a leucine (Leu or L) at the 27-position.
The alanine at the 8th position enhances bioavailability but the other two amino substitutions are made to enhance the manufacturing process (i.e. create manufacturing stability).
For use in vivo, in humans, the GHRH analog known as CJC w/o the DAC or tetra (4) substituted GRF(1-29) or modified GRF(1-29) is a very effective peptide with a half-life probably 30+ minutes.
That is long enough to be completely effective.
The saturation dose is also defined as 100mcg.
Problem w/ Using any GHRH alone
The problem with using a GHRH even the stronger analogs is that they are only highly effective when somatostatin is low (the GH inhibiting hormone). So if you unluckily administer in a trough (or when a GH pulse is not naturally occurring) you will add very little GH release. If however you luckily administer during a rising wave or GH pulse (somatostatin will not be active at this point) you will add to GH release.
Solution is GHRP + GHRH analog
The solution is simple and highly effective. You administer a GHRH analog with a GHRP. The GHRP creates a pulse of GH. It does this through several mechanisms. One mechanism is the reduction of somatostatin release from the hypothalamus, another is a reduction of somatostatin influence at the pituitary, still another is increased release of GHRH from the brain and finally GHRPs act on the same pituitary cells (somatotrophs) as do GHRHs but use a different mechanism to increase cAMP formation which will further cause GH release from somatotroph stores.
GHRH also has a way of reciprocally reinforcing GHRPs action.
The result is a synergistic GH release.
The GH is not additive it is synergistic. By that I mean:
If GHRH by itself will cause a GH release valued at 2
and GHRP itself will cause a GH release valued at 5
Together the GH is not 7 (5+2) it turns out to say 16!
A solid protocol
A solid protocol would be to use a GHRP + a GHRH analog pre-bed (to support the nightime pulse) and once or twice throughout the day.
For anti-aging, deep restful restorative sleep, the once at night dosing is all you need. For an adult aged 40+ it is enough to restore GH to youthful levels.
However for bodybuilding or fatloss or injury repair multiple dosings can be effective.
The GHRH analog can be used at 100mcg and as high as you want without problems.
The GHRP-2 can always be used at 100mcg w/o problems but a dose of 200mcg will probably be fine as well.
Again desensitization is something to keep an eye on particularly with the highest doses of GHRP-2 and all doses of Hexarelin.
So 100 - 200mcg of GHRP-2 + 100 - 500mcg+ of a GHRH analog taken together will be effective.
This may be dosed several times a day to be highly effective.
A solid approach is a bit more conservative at 100mcg of GHRP-2 + 100mcg of a GHRH analog dosed either once, twice, three or four times a day.
When dosing multiple times a day at least 3 hours should separate the administrations.
The difference is once a day dosing pre-bed will give a youthful restorative amount of GH while multiple dosing and or higher levels will give higher GH & IGF-1 levels when coupled with diet & exercise will lead to muscle gain & fatloss.
Dose w/o food
Administration should ideally be done on either an empty stomach or with only protein in the stomach. Fats & carbs blunt GH release. So administer the peptides and wait about 20 minutes (no more then 30 but no less then 15 minutes) to eat. AT that point the GH pulse has about hit the peak and you can eat what you want.
Phatbastard
Knowledge Equals Results
This actually old INFO^^^^^^^^^^^^^^^^^ it has been shown that GHRPS can be utilized at higher dosages with efficacy! Think thats a word LOL. You guys are doing a great job with this thread. I would look into the newer data on this one though. I'f I run across it I will check to see if it has been posted yet.
vibrant
CHEMICALLY ENGINEERED
I know the topic on folli is controversial right now but anyway here's some info:
Follistatin 344
You can nag your dealer until he pins you on to the fender of his SUV, but you still won't get any. We're talking about the anabolic wonder stuff that researchers at Ohio State University are doing experiments with. A single injection will change you for the rest of your life into a hulk of the kind that Markus Ruehl [see photo below] would say: that much muscle just isn't aesthetic.
The super steroid in question is not a hormone. It's a common-cold virus that the researchers have made some adjustments
to. Viruses invade cells and release their genes into them. Then the cell obeys the virus genes instructions, and makes the proteins according to the genes blueprint. The proteins formed are the building blocks for new viruses.
The researchers managed to get their viruses to program the muscle cells to make proteins that deactivated the myostatin protein. Myostatin is a protein that muscle cells make to prevent fitness center owners from having to change jobs and become SUV salesmen.
Not that the researchers had something against fitness center owners. They are looking for a cure for muscular dystrophy. In their study, which was published in the prestigious PNAS, they tested three myostatin inhibiting genes: the gene for growth and differentiation factor-associated serum protein-1 (GASP-1), follistatin-related gene (FLRG) and the gene for follistatin-344 (FS).
There are various kinds of follistatin and they all have different functions. As far as we know, only follistatin-344 is active in muscle tissue.
The mice in the experiment were given an injection when they were four weeks old. The photos below show their musculature two years later. AAV1 stands for the adenovirus that the researchers used. AAV1-GFP was the control group.
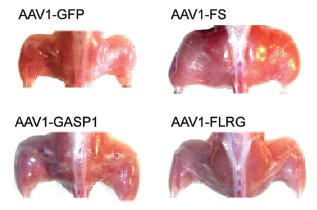
The injection with the gene for follistatin-344 was the most effective. This becomes clearer if you look at the figure below, which shows the weight of the mice two years after the injection.
But most beautiful of all is the graph below. This shows how the mice's power developed over their lifespan. The mice in the control group the green curve get weaker towards the end of their life. But the mice that were injected with AAV1-FS the red curve just keep on getting stronger.
The researchers obtained the same success when they injected the viruses into mice that had congenital muscle disease. "The striking ability of FS to provide gross and functional long-term improvement to dystrophic muscles in aged animals warrants its consideration for clinical development to treat musculoskeletal diseases, including older DMD patients", they write.
Only a few years, and muscular diseases will be a thing of the past. And all fitness centres will go bust.
Sources:
Long-term enhancement of skeletal muscle mass and strength by single gene administration of myostatin inhibitors
Follistatin 344
You can nag your dealer until he pins you on to the fender of his SUV, but you still won't get any. We're talking about the anabolic wonder stuff that researchers at Ohio State University are doing experiments with. A single injection will change you for the rest of your life into a hulk of the kind that Markus Ruehl [see photo below] would say: that much muscle just isn't aesthetic.
The super steroid in question is not a hormone. It's a common-cold virus that the researchers have made some adjustments
to. Viruses invade cells and release their genes into them. Then the cell obeys the virus genes instructions, and makes the proteins according to the genes blueprint. The proteins formed are the building blocks for new viruses.
The researchers managed to get their viruses to program the muscle cells to make proteins that deactivated the myostatin protein. Myostatin is a protein that muscle cells make to prevent fitness center owners from having to change jobs and become SUV salesmen.
Not that the researchers had something against fitness center owners. They are looking for a cure for muscular dystrophy. In their study, which was published in the prestigious PNAS, they tested three myostatin inhibiting genes: the gene for growth and differentiation factor-associated serum protein-1 (GASP-1), follistatin-related gene (FLRG) and the gene for follistatin-344 (FS).
There are various kinds of follistatin and they all have different functions. As far as we know, only follistatin-344 is active in muscle tissue.
The mice in the experiment were given an injection when they were four weeks old. The photos below show their musculature two years later. AAV1 stands for the adenovirus that the researchers used. AAV1-GFP was the control group.
The injection with the gene for follistatin-344 was the most effective. This becomes clearer if you look at the figure below, which shows the weight of the mice two years after the injection.
But most beautiful of all is the graph below. This shows how the mice's power developed over their lifespan. The mice in the control group the green curve get weaker towards the end of their life. But the mice that were injected with AAV1-FS the red curve just keep on getting stronger.
The researchers obtained the same success when they injected the viruses into mice that had congenital muscle disease. "The striking ability of FS to provide gross and functional long-term improvement to dystrophic muscles in aged animals warrants its consideration for clinical development to treat musculoskeletal diseases, including older DMD patients", they write.
Only a few years, and muscular diseases will be a thing of the past. And all fitness centres will go bust.
Sources:
Long-term enhancement of skeletal muscle mass and strength by single gene administration of myostatin inhibitors
Last edited:
Phatbastard
Knowledge Equals Results
Are you referring to "booming" or "mega dosing"? If I remember correctly,i think that's the term they used...
Don't recall it being called that. But it's been shown doses in the 400mcg range to be more affective than the before thought of the 100mcg saturation dose. I don't want to say much more with out the evidence to back it up but it's becoming more popular to run higher doses as we go along.
Ezskanken
New member
Yup, you are correct there. It's sometimes referred to as what I mentioned. If you don't mind posting up where you read that I would love to take a look at at. I can always use evidence from both sides of the fence...
Don't recall it being called that. But it's been shown doses in the 400mcg range to be more affective than the before thought of the 100mcg saturation dose. I don't want to say much more with out the evidence to back it up but it's becoming more popular to run higher doses as we go along.
Phatbastard
Knowledge Equals Results
I will if I run across it! Just thought I would let you know it's not a big intrest to me but I know its out there.
Similar threads
- Replies
- 15
- Views
- 6K
- Replies
- 147
- Views
- 70K